

Hospital Protocol: Management of Umbilical Cord Prolapse
Purpose: To provide a clear, evidence-based, stepwise approach for the recognition and management of umbilical cord prolapse (UCP), aiming to reduce perinatal morbidity and mortality through timely and appropriate intervention.
Scope: Applies to all obstetric and neonatal care providers (obstetricians, anesthetists, midwives, nurses, neonatologists, support staff) working in labour ward, operating theatre, and related obstetric emergency settings.
Definitions:
Umbilical cord prolapse (UCP): descent of the umbilical cord through the cervix, below or alongside the presenting part, after rupture of membranes.
Occult cord prolapse: cord lies alongside presenting part but not palpable/visible beyond cervix; suspected if unexplained fetal heart rate abnormalities occur.
Risk Factors: Malpresentation (breech, transverse, oblique), unengaged or high presenting part (especially at ROM), polyhydramnios, multiple pregnancy, preterm labour, long cord, iatrogenic causes (AROM with high head, internal manipulations, external cephalic version).
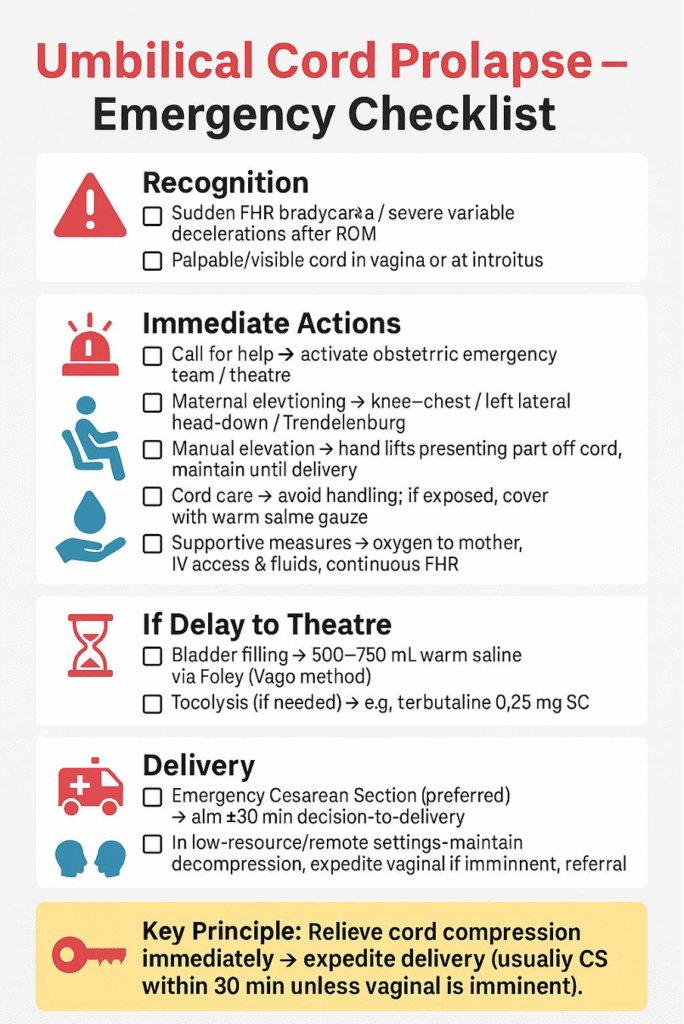
Recognition: Clinical: visible or palpable cord at or beyond the cervix/vagina. Fetal monitoring: sudden prolonged deceleration, severe variable decelerations, or sustained bradycardia after ROM.
Responsibilities:
First responder (midwife/doctor): Recognize, call for help, initiate immediate maneuvers.
Team leader (obstetrician): Direct management, decide delivery mode, document times.
Anaesthetist: Prepare for urgent cesarean section.
Neonatal team: Prepare for potential resuscitation.
Nursing/midwifery staff: Assist with positioning, IV access, monitoring, transfer to theatre.
Procedure (Stepwise Management):
Immediate Actions: Call for help → activate obstetric emergency team & prepare theatre. Maternal positioning → knee–chest, left lateral with head down (exaggerated Sims), or Trendelenburg. Manual elevation of presenting part with gloved hand until definitive delivery. Cord care → minimize handling; if protruding, cover with warm saline-soaked gauze. Adjuncts if delay to theatre: bladder filling: 500–750 mL warm saline via Foley (Vago method), consider tocolysis (e.g., terbutaline 0.25 mg SC). Supportive measures: oxygen by mask, IV access, IV fluids, continuous FHR monitoring if feasible.
Definitive Delivery: Emergency cesarean section is the treatment of choice. Decision-to-delivery interval (DDI) aim ≤30 minutes. If vaginal delivery imminent (full dilatation, head on perineum): expedite by instrumental delivery (vacuum/forceps). WHO/low-resource setting: if cesarean unavailable, maintain decompression and expedite vaginal birth if possible; urgent referral.
Post-delivery Care: Neonatal resuscitation team present at delivery. Maternal postoperative/postnatal care as per routine. Document: time of diagnosis, maneuvers used, decision time, delivery time, neonatal outcome.
Audit & Quality Assurance: Audit criteria: time from diagnosis to delivery (target ≤30 minutes), perinatal outcomes (Apgar, neonatal admission, cord pH), compliance with maneuvers (positioning, manual elevation, bladder filling if delay). Debrief: clinical team and parents after event. Training: regular multidisciplinary emergency drills for UCP.
References: RCOG Green-top Guideline No. 50: Umbilical Cord Prolapse (2022), ACOG Practice Bulletin: Obstetric Emergencies / Intrapartum Care, SOGC Clinical Practice Guidelines, WHO: Managing Complications in Pregnancy and Childbirth.
Compiled By:
Dr. Tanjila Karim
Contributors
- Prof Dr Fawzia Hossain
- Dr Tanjila Karim
- Dr Maniza Khan
- Dr Lata Dutta
- Dr Ananna Zakia
- Dr Lutfa Amin
- Dr Tasrina Akhter
- Dr Amrita Saha
- Dr Shanjida Kabir
- Dr Aklima Zakaria Zinan
