

Introduction
• Thyroid disease is a common endocrine disorder in women of childbearing age.
• Both inadequate and excessive treatment of thyroid disorders, the choice of treatment, as well as delayed commencement and adjustment of treatment, can result in detrimental effects on the pregnancy and fetus.
Thyroid Physiology in Pregnancy & Diagnostic Considerations
• Pregnancy causes physiologic changes in thyroid hormone dynamics and regulation: e.g. increased thyroid binding globulin (TBG), hemodilution, increased renal iodine clearance, and the thyrotropic effect of B-hCG (which can transiently suppress TSH in first trimester).
• Because of these changes, standard nonpregnant reference ranges for TSH/free T4 may not apply; trimester specific reference ranges or pregnancy adjusted cutoffs should be used.
• Ideally, preconception measurement of TSH (and where relevant T4/antibodies) is recommended in women with known thyroid disease or risk.
Iodine Intake
• All pregnant and breastfeeding women should have a total daily intake of approximately 200–250μg iodine.
• Consideration should be given to increasing dietary intake of iodine-rich foods or consuming daily oral supplementation of 150μg iodine in the form of potassium iodide (started 3 months in advance or as soon as possible in pregnancy).
Screening Strategy
• RCOG does not mandate universal screening of all pregnant women for thyroid dysfunction; instead, targeted case-finding is recommended.
• Risk factors prompting testing may include: personal history of thyroid disease, goitre, symptoms suggestive of thyroid dysfunction, positive thyroid antibodies, type 1 diabetes or other autoimmune disease, infertility, history of miscarriages, or other high-risk features.
• Subpopulations with specific risk factors who are known to have a higher prevalence of overt thyroid disorders should be tested for thyroid dysfunction as soon as possible in pregnancy, preferably in the first trimester.
Hypothyroidism in Pregnancy
This includes both overt and subclinical forms.
Overt Hypothyroidism (elevated TSH + low free T4)
Subclinical Hypothyroidism (elevated TSH, normal free T4)
Pre-conceptional
• Untreated or undertreated overt hypothyroidism is associated with miscarriage, preterm birth, preeclampsia, low birthweight, and neurodevelopmental impairment in the child.
• Target TSH ≤ 2.5 mU/L for women with known hypothyroidism (overt or subclinical) who are planning pregnancy.
• RCOG suggests increasing by about 25-30% immediately when pregnancy is confirmed. It can be achieved by:
- doubling the dose of levothyroxine on 2 days of each week.
- implementing a dose increment of:
• 25μg per day for women taking 100μg or less levothyroxine daily
• 50μg per day for women taking greater than 100μg levothyroxine daily
During Pregnancy
Women with pre-existing overt hypothyroidism
• Increase LT4 dose (by ~25-30%) as soon as pregnancy is confirmed.
• Monitor thyroid function regularly (every 4-6 weeks initially).
• Maintain target TSH ≤ 2.5 mU/L (or within pregnancy-/trimester-specific reference ranges).
Newly diagnosed overt hypothyroidism
• Start LT4 as soon as possible.
• Suggested starting dose ~1.6 µg/kg/day in severe cases / overt disease.
• Repeat thyroid function tests in ~4 weeks to adjust.
Subclinical hypothyroidism (SCH) (pregnant women)
• Consider LT4 in SCH, especially if TSH is high (e.g. > upper limit of normal or >10 mU/L) or if there are other risk factors (autoantibodies, miscarriages, fertility issues).
• Lower intensity treatment (doses ~1.0-1.2 µg/kg/day) may be used.
• When not treating, monitor TSH free T4 every 4-6 weeks up to ~20 weeks, and again around ~28 weeks.
LT4 Dose Adjustment Protocol
• As pregnancy progresses, LT4 requirements increase, due to increased thyroid binding proteins, increased metabolic demand, etc.
• Empirical dose increases early help avoid hypothyroid periods.
• Avoid overtreatment to prevent maternal/fetal hyperthyroid risks.
Recommendations
• In women with infertility or recurrent miscarriage, LT4 may be considered in subclinical hypothyroidism (especially if TSH > ~2.5 mU/L).
• If TSH is only mildly elevated (e.g. ≤4 mU/L) and the woman is antibody-negative, LT4 may be withheld and thyroid function monitored.
• In women who are TPO antibody–positive and have a TSH in the mildly elevated range (e.g. 2.5–4), LT4 therapy may be considered.
Hyperthyroidism in Pregnancy
This primarily concerns Graves’ disease and gestational transient thyrotoxicosis.
Graves’ Disease
• Untreated hyperthyroidism in pregnancy increases risks of miscarriage, preterm birth, preeclampsia, heart failure, fetal loss, and fetal/neonatal thyrotoxicosis.
• Management should balance maternal control with minimizing fetal exposure to antithyroid drugs (ATDs).
• A multidisciplinary team (obstetrician, endocrinologist) should be involved.
Pre-Conceptional
• Pre-pregnancy counselling is recommended in women with hyperthyroidism to minimise maternal and fetal adverse outcomes.
• The option of definitive treatment with radioactive iodine or thyroidectomy should be discussed, especially in women with more severe disease.
• Following definitive treatment, women should wait at least 6 months before attempting to conceive. They should also have had serum fT4 within the reference range on two measurements 3 months apart.
• A persistently increased TSH-receptor antibody (TRAb) level (usually taken as greater than 3 times the threshold for positivity) assessed around 6 months post-treatment is associated with increased risk of fetal Graves’ disease and consideration may be given to further delay conception.
• Hyperthyroidism requiring treatment with antithyroid drugs while trying to conceive should use propylthiouracil (PTU).
During Pregnancy
• When pregnant, where a woman with a history of hyperthyroidism has been euthyroid for 6 months or more on low dose of an antithyroid drug (CMZ < 10 mg or PTU < 200 mg daily), consider discontinuing drugs with close thyroid function monitoring.
• If antithyroid drug treatment is required:
- First trimester: Prefer propylthiouracil (PTU), because methimazole (or carbimazole) is associated with rare embryopathy in first trimester.
- Second/third trimesters: After first trimester, switching to methimazole / carbimazole is usually preferred because of lower risk of maternal hepatotoxicity with methimazole vs PTU.
• If a woman conceives on CMZ a switch to PTU should be made as soon as possible before 10 weeks gestation, with an advised dose ratio of 1:20 (CMZ:PTU). No benefit of switching to PTU if a woman presents after 10 weeks.
• Monitoring: During 1st trimester monitor every 2–4 weeks with measurement of serum TSH and fT4. After 20 weeks of pregnancy every 4–8 weeks.
• When stopping antithyroid drug treatment, when switching between antithyroid drugs and following dose adjustments, consider fortnightly testing.
• TRAb measurement in the first trimester is recommended in all women with a history of Graves’ disease, even following definitive treatment. If it is above the threshold for positivity (e.g. >3× upper limit) or if the woman is on antithyroid drugs, a further measurement at 20 and 28 weeks of gestation is recommended.
• Target level: Titration of antithyroid drugs should target fT4 concentrations in the upper half of reference range.
Fetal Considerations
• RCOG emphasize that maternal antibodies (e.g. TSH receptor antibodies) cross the placenta and may influence fetal thyroid function; thus, fetal monitoring is recommended if risk is present.
• Serial ultrasound scans to assess fetal biometry (e.g. fetal tachycardia, growth abnormalities, goitre) with umbilical artery Doppler at monthly intervals from 26 to 28 weeks is recommended in those who at any time during pregnancy had uncontrolled Graves’ disease, required antithyroid drug treatment or had a TRAb level three times above the threshold.
Post-pregnancy
• Neonates of women with known Graves’ disease, of those receiving antithyroid medication during pregnancy and those with increased TRAb levels should have their thyroid function monitored soon after birth and at 1–2 weeks post-birth.
• A thyroid function test is recommended 6–8 weeks after birth in women with a history of pre-existing hyperthyroidism.
• Both CMZ and PTU are considered safe during breastfeeding in lowest effective dose.
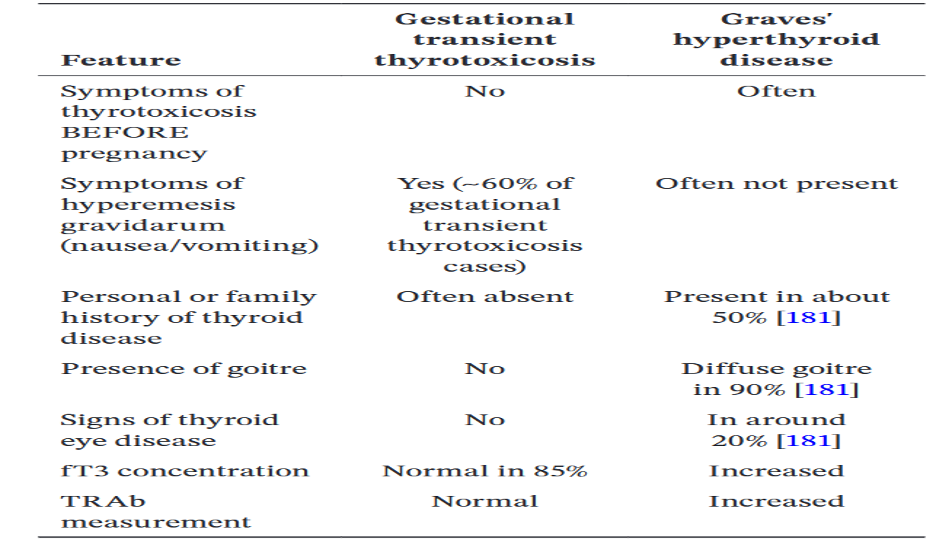
Gestational Transient Thyrotoxicosis
• With the new finding of a suppressed serum TSH accompanied by an increased fT4 concentration in pregnancy, we should separate Graves’ disease from gestational transient thyrotoxicosis using a range of clinical features and measurements of TRAb and fT3.
• Gestational transient thyrotoxicosis requires symptomatic and supportive management only.
Thyroid Nodules and Thyroid Cancer
• New onset thyroid nodule or goitre in pregnancy – check thyroid function and refer to specialist.
• If there is suspicion of malignancy on ultrasound, a FNAC can be performed at any gestation.
• Thyroid surgery (thyroidectomy) is reserved for women who cannot tolerate ATDs or have large goitres / compression symptoms; best done between 14 to 22 weeks.
• Radioactive iodine (RAI) is contraindicated in pregnancy and also in breastfeeding; should not be given.
• Counsel no change in survival or recurrence rate due to pregnancy.
• Anesthetist review in case of enlarged thyroid in pregnancy.
Postpartum Thyroiditis (PPT)
• PPT is defined as the development of thyroid dysfunction, excluding other thyroid diseases, within the first 12 months following a pregnancy in a previously euthyroid woman.
• This is an autoimmune disorder associated with antibodies to TPO and thyroglobulin caused by a reactivation of the immune system following the relative immune suppression during pregnancy.
• For women with postpartum thyroiditis, management is symptomatic (beta blockers, etc.) during the thyrotoxic phase; in the hypothyroid phase, LT4 may be used if symptomatic or TSH markedly elevated.
Compiled By:
Dr. Arefin Arif
Contributors
- Prof Fauzia Hossain
- Prof Tabassum Parveen
- Dr Raunak Jahan Koly
- Dr Arifa Sharmin Maya
- Dr Taslima Akter
- Dr Pollobi Shaha
- Dr Israt Jahan
- Dr Amrita Saha
- Dr Anika Tasnia
- Dr Farzana Haque
- Dr Luthfa Amin
- Dr Nafisa Jafreen
- Dr Fatema Yesmin
- Dr Afroza Akter
- Dr Farjana Sultana
