

Chapter -2025
Purpose of the Guidelines
These guidelines provide evidence-based recommendations for evaluating and managing male
infertility in Bangladesh. Male factors contribute to nearly half of all infertility cases, and
accurate assessment is key to guiding treatment and avoiding unnecessary interventions for the
female partner.
They aim to:
Outline a systematic approach to history-taking, physical examination, and diagnostic
testing.
Guide medical and surgical treatments, and define the role of IUI, IVF, and ICSI in male
factor infertility.
Address health and genetic implications of specific conditions, including serious
systemic disorders.
Support individualized, evidence-based care without replacing clinical judgment.
Recommendations are based on structured literature review using the PICO framework and are
intended for urologists, gynecologists, and fertility specialists. They serve as guidance, not rigid
clinical standards, and remain valid for up to five years or until the next update.
Methodology
Development of the Bangladesh Guidelines for Male Infertility (2025, RCOG Bangladesh
Chapter) involved topic assignment, systematic review, and multidisciplinary expert discussions
among urologists, andrologists, and reproductive medicine specialists.
A comprehensive literature search (PubMed, Cochrane, Medline, Index Copernicus, Embase)
emphasized South Asian studies, especially from India and Bangladesh, to ensure regional
relevance. Reference sources included ASRM and RCOG guidelines.
Keywords covered: etiology, prevalence, semen analysis, azoospermia, sperm retrieval,
hypogonadism, infection, genetics, varicocele, cryopreservation, and idiopathic infertility. Only
English-language human studies were included.
Each chapter begins with evidence-based recommendations, followed by discussion and
clinical flowcharts adapted to local practice.Recommendation grading:
Strong/Moderate/Weak — per ASRM levels of confidence.
Clinical Principle (CP) — widely accepted best practice even without strong evidence.
Expert Opinion (EO) — consensus where data are limited, especially for Bangladesh.
This guideline adapts international standards to Bangladeshi socio-economic and cultural
contexts, addressing local constraints, delayed presentation, and the central importance of
family-building.
Introduction
Infertility exerts a major psychosocial burden in Bangladesh, where childbearing is closely
linked to social acceptance, family stability, and women’s societal standing. It has become a
public health priority under the national reproductive health agenda.
Several Bangladesh-specific challenges complicate management:
Limited access to reliable semen analysis and diagnostic facilities.
Unregulated growth of fertility and IVF centers.
Frequent neglect of male partner evaluation in infertile couples.
Scarcity of trained andrology services with microsurgical capacity.
High cost of diagnostics and ART, placing them beyond reach for most patients.
Lack of structured infertility training in medical curricula, leading to low clinical
competence and public awareness.
In contrast, ASRM and RCOG guidelines emphasize a stepwise, evidence-based evaluation of
both partners, standardized laboratory quality control, appropriate ART use, and clinician
accreditation (ASRM, 2023; RCOG, 2022). Adapting these best practices to Bangladesh’s
socioeconomic realities—with focus on affordability, regulation, and education—is critical.
Developing national guidelines that localize ASRM and RCOG principles can enhance
awareness, standardize clinical practice, and gradually reduce the burden of infertility in
Bangladesh.
Commonly Used Terms in Semen Analysis
to failure of seminal fluid production
No sperm in the ejaculate, caused either by blockage in the genital tract
| Term Definition | |
| Aspermia | Absence of ejaculate, usually due or obstruction of the reproductive tract. |
| Azoospermia |
Oligozoospermia Asthenozoospermia Teratozoospermia Normozoospermia Retrograde
Ejaculation
| (obstructive) or defective sperm production (non-obstructive). | |
| Low sperm count in the ejaculate. | |
| Impaired sperm motility, where a considerable proportion of sperm show weak or abnormal movement, limiting fertility. | |
| Predominance of sperm with abnormal morphology, potentially compromising fertility. | |
| Ejaculate with normal semen parameters including sperm count, motility, morphology, and volume, consistent with optimal fertility potential. | |
| A condition where semen flows backward into the bladder rather than through the urethra during ejaculation, decreasing fertility. |
GUIDELINE STATEMENTS
DEFINITION
“Infertility is the inability of a sexually active, non-contracepting couple to achieve spontaneous
pregnancy in 1 year.”
Epidemiology and aetiology
| Recommendation Strength | |
| To categorize infertility, both partners should be investigated simultaneously. | Moderate |
| There are no reliable figures for the global prevalence of infertility. It is estimated to be 8%–12%, of which only the male partner accounts for 20%, females for 38%, mixed for 27%, and unknown for 15%. In India, the rate varies from 3.9% to 16.8%, with significant variations not only across different states but also within the same region among various castes and tribes. | – |
| The primary cause of infertility could be defined in only 40%. They are grouped into three categories: nonobstructive, obstructive, and coital.[ Raheem AA et al.,2011] In 75% of cases of oligospermia, the reasons remained unknown. | – |
Infertility is a global public health concern, affecting about 15% of married couples worldwide
[Sharlip ID, 2002]. Male factors contribute to 20–40% of cases [George SS, 2003; Sigman M,
1997]. The WHO estimates that 60–80 million couples are affected globally [Mascarenhas MN,2012; Boivin J, 2007; Rutstein, 2004], with prevalence varying by region [Sciarra J, 1994]. The
issue is often greatest in high-fertility countries, described as the paradox of “barrenness amid
plenty” [Population Council, 2004; van Balen F, 2001].
In South Asia, data from India indicate that male factors account for about 23% of infertility
cases among couples seeking treatment [Mascarenhas MN, 2012]. Up to 50% of infertility may
relate to male reproductive disorders, and about 25% of cases remain unexplained despite
evaluation [Boivin J, 2007].
In Bangladesh, while precise prevalence data are limited, available studies suggest a
comparable burden to neighboring countries. The condition carries dual challenges — social
stigma surrounding childlessness and limited access to specialized male infertility care. Despite
cultural tendencies to attribute infertility to women, evidence confirms that male factors are a
major contributor.
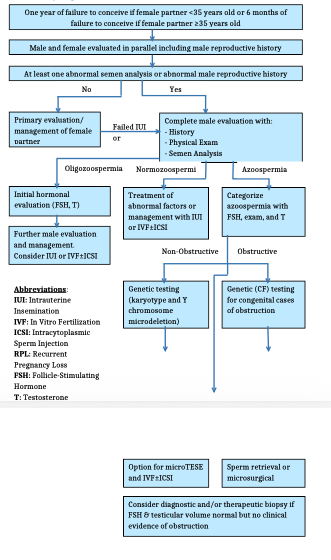
Both ASRM and RCOG guidelines stress evaluation of the male partner in every infertile couple.
They recommend a structured diagnostic approach involving semen analysis, hormonal testing,
and imaging to classify infertility into three groups [van Balen F, 2001]:
1. 2. Non-obstructive causes – testicular failure, hormonal dysfunction, genetic defects.
Obstructive causes – congenital or acquired reproductive tract blockage.
3. Coital or ejaculatory dysfunction.
Adapting these frameworks to the Bangladeshi context is essential to ensure accurate
diagnosis, promote equitable care, and lessen the psychological and social burden
disproportionately placed on women. Establishing national protocols aligned with ASRM and
RCOG standards would markedly improve male infertility management and strengthen
reproductive health services.
Evaluation and semen analysis
| Recommendation: Strength | |
| Evaluation of both partners should be conducted simultaneously. | Moderate |
| A detailed reproductive history and targeted clinical examination are essential. | Strong |
| Semen analysis must be carried out according to the WHO Laboratory Manual for the Examination and Processing of Human Semen, 6th edition reference criteria [WHO.;2022]. | Strong |
| Endocrine profile testing should be offered only if semen analysis is abnormal in at least two separate tests. | Strong |
| Scrotal ultrasound is recommended for patients who are obese, have a history of scrotal surgery, or present with a small, tight scrotum. | moderate |
| Transrectal ultrasound should be performed only when there is suspicion of ejaculatory duct obstruction. | Strong |
| In cases of non-palpable vas deferens, congenital bilateral absence of vas deferens (CBAVD) should be suspected, and both partners should undergo CFTR mutation testing. | Strong |
| Diagnostic testicular biopsy should preferably be done in centers equipped for sperm retrieval and cryopreservation. | Strong |
| Vasography should not be used solely as a diagnostic test; it is only indicated intraoperatively before reconstructive surgery. | Strong |
In Bangladesh, evaluation of male infertility begins with a detailed clinical history and physical
examination. Particular focus should be placed on sexual dysfunction [Lotti F, 2011] and timing
of intercourse, as improper timing often contributes to subfertility. Couples are advised to have
intercourse every other day from five days before to five days after expected ovulation to
optimize conception chances [Smith RP, 2014]. Given that socio-economic disparities strongly
affect healthcare access and compliance, socio-economic assessment is essential in every
evaluation [Kulkarni G, 2014]. Clinical examination must also exclude infections [Das P, 2008],
particularly genitourinary tuberculosis, which remains relatively prevalent in South Asia,
including Bangladesh [Kapoor R, 2008].
Semen analysis is the cornerstone of male infertility evaluation, following ASRM, RCOG, and
OGSB (Bangladesh) guidelines. Because of intra-individual variability, two semen analyses
spaced at least two weeks apart are required [ASRM, 2006]. The ideal abstinence period is 2–5
days, consistent with ASRM and WHO recommendations [Hanson BM, 2018]. Measurement of
seminal fructose is no longer considered a reliable marker to differentiate obstructive from
non-obstructive azoospermia.
For abnormal semen results, second-line investigations should include FSH, LH, and total
testosterone, with estradiol, SHBG, and prolactin added as needed [Hotaling JM, 2014]. In
Bangladesh, FSH remains the preferred marker of spermatogenesis due to cost and limited
access to inhibin B assays.
Advanced semen tests—including sperm DNA fragmentation, reactive oxygen species, and
antisperm antibody assays—remain optional [Zini A, 2011; Dutta S, 2020]. Both ASRM and
RCOG highlight their limited clinical utility and high cost in resource-constrained settings. The
WHO Laboratory Manual (6th Edition, 2021) underscores that semen analysis cannot
definitively classify fertility status; instead, decision limits now guide management. This
pragmatic approach is especially relevant in Bangladesh, where delayed diagnosis and
treatment often worsen outcomes.
| Semen Normal Borderline Pathological | |||
| Count | 10-20 million./ml | <10 mill./ml | |
| Motility (Progressive) | 35-49% | < 35% | |
| Progressive Motility | |||
| Morphology | 4-13% | <4% | |
| Sperm antibody binding (Agglutination) | 50-79% | >80% | |
Sperm DNA fragmentation (SDF) and ROS testing are considered extended investigations with
potential but non-routine clinical use, remaining largely within the research domain under
ASRM and RCOG recommendations.
>20 mill./ml 50% >14 % <50% Azoospermia: Evaluation and Management in the Context of Bangladesh
| Obstructive azoospermia Recommendation: | Strength |
| In men with non-palpable vas deferens, congenital bilateral absence of vas deferens (CBAVD) should be considered, and CFTR mutation testing is recommended. | Strong |
| Diagnostic testicular biopsy is best performed in centers with facilities for both sperm retrieval and cryopreservation. | moderate |
| Vasography should not be used solely for diagnostic purposes; it should only be carried out intraoperatively before reconstructive procedures. | Strong |
| Men whose female partners have good ovarian reserve and who present with azoospermia due to epididymal or vasal obstruction should be offered microsurgical vasovasostomy or epididymovasostomy [Gautam G et al.;2005]. | Strong |
| In cases of CBAVD [38], or when the female partner has reduced ovarian reserve, sperm retrieval techniques such as MESA, TESE, PESA, or TESA are recommended. | Strong |
| Sperm retrieval techniques may also be used in conjunction with reconstructive surgery when indicated. | Strong |
| For patients with irreparable reproductive tract obstruction, sperm retrieval combined with ICSI/IVF should be considered. | Strong |
| Men with ejaculatory duct obstruction (EDO) and dilated ejaculatory ducts may benefit from transurethral resection of the ejaculatory ducts (TURED). [Surya BV et al.;1988] | moderate |
| Men with suspected EDO but normal TRUS findings are likely to have fibrous, post- | Strong |
| infective ejaculatory duct obstruction. These patients are not candidates for TURED and instead should undergo PESA with ICSI |
| Recommendation: Strength | |
| Men with non-obstructive azoospermia (NOA) and sperm counts below 5 million/ml should undergo a thorough evaluation, including detailed medical history, hormonal profile, and genetic testing (karyotyping and Y-chromosome microdeletion analysis) to determine the underlying cause [Clementini E et al.;2005]. | |
| In cases with complete AZFa or AZFb microdeletions, surgical sperm retrieval is contraindicated [Arshad MA et al.;2015]. | |
| Young men with AZFc deletions should receive genetic counseling about the potential transmission of the defect to offspring. These patients have relatively higher success rates for sperm retrieval (up to 55%) when treated with microdissection TESE (mTESE). | |
| Microdissection TESE is considered the most effective method for sperm retrieval in NOA [Shah R,2018]. | |
| Testosterone replacement therapy should not be used as a treatment for infertility. | |
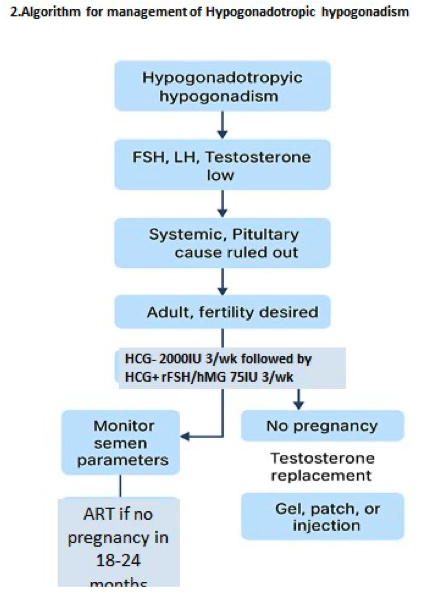
| Hypogonadotropic hypogonadism | |
| Recommendation: Strength | |
| Male hypogonadotropic hypogonadism (HH) is characterized by impaired testicular production of both androgens and sperm, resulting from congenital or acquired disorders involving the hypothalamus and/or pituitary gland [Fraietta R,2013]. | |
| Diagnosis should be based on low serum FSH, LH, and testosterone, with MRI/CT of the brain as part of the evaluation. | |
| Clinical features vary depending on the age at which presentation occurs. [Young J,2019] | |
| Androgen replacement therapy should be offered when fertility is not desired. | |
| For fertility induction, gonadotropin therapy should be initiated to stimulate spermatogenesis. [Hayes FJ,1998] | |
| Testosterone replacement therapy must not be used as a treatment for infertility. [Ohlander SJ,2016] | |
| HH is one of the rare conditions in which specific medical therapy can successfully reverse infertility.[ Han TS,2010] | |
| Azoospermia, the absence of spermatozoa in the centrifuged semen pellet, should be | |
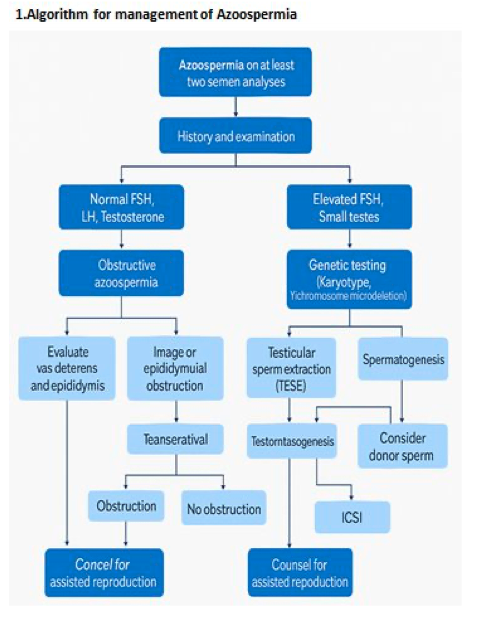
Nonobstructive azoospermia
confirmed by two separate semen analyses [ASRM, 2019]. Obstructive azoospermia (OA)
accounts for 20–40% of cases, while non-obstructive azoospermia (NOA) is more prevalent
globally, including in Bangladesh. Evaluation should identify the site and cause of obstruction.According to ASRM and RCOG guidelines, surgical correction is recommended when feasible
and the female partner’s ovarian reserve is adequate [Namekawa T, 2018].
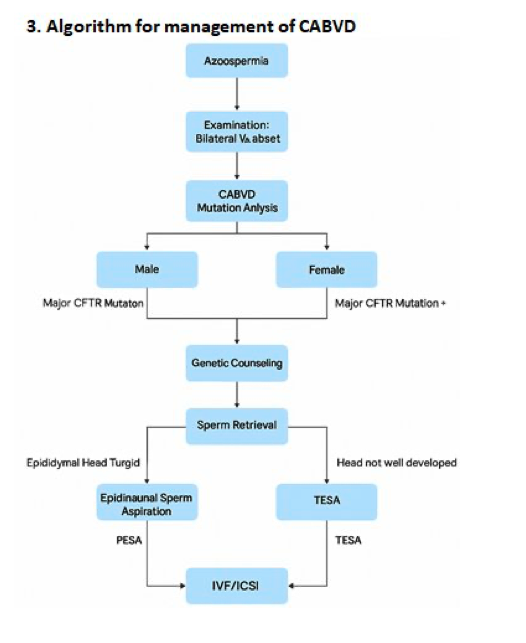
Low semen volume, acidic pH, and absent fructose indicate OA, commonly due to congenital
bilateral absence of the vas deferens (CBAVD) or ejaculatory duct obstruction (EDO). CBAVD is
diagnosed by bilateral absence of vasa on palpation. CFTR gene mutation testing and partner
carrier screening are essential to prevent cystic fibrosis. In Bangladesh, such testing is limited to
tertiary centers. Sperm retrieval in CBAVD is typically successful via epididymal (PESA/MESA)
or testicular aspiration (TESA) techniques.
In NOA, elevated FSH (>2.5× normal) is strongly predictive, though normal values do not
exclude it. Low inhibin B (<170 pg/mL; IQR 125–215 pg/mL) also supports the diagnosis
[Barbotin AL, 2020]. 17-hydroxyprogesterone helps assess intratesticular testosterone.
Karyotyping and Y-chromosome microdeletion testing should precede sperm retrieval, per
ASRM/RCOG guidance.
Selected NOA cases may benefit from medical therapy. Clomiphene citrate and hCG can raise
intratesticular testosterone and stimulate Leydig cell function. In hypogonadotropic
hypogonadism (HH)—characterized by low FSH, LH, and testosterone—fertility may be
restored with gonadotropin therapy; testosterone replacement is used when fertility is not
desired [Ohlander SJ, 2016].
Cryptorchidism remains prevalent in Bangladesh, especially in rural areas with delayed
presentation. Testicular biopsy during orchiopexy helps exclude malignancy. Early orchiopexy
(<12 months) preserves spermatogenesis, while delayed surgery reduces sperm production. In
azoospermic men, TESE may yield sperm for assisted reproduction. In Klinefelter syndrome,
micro-TESE achieves sperm retrieval rates of 22–50%, consistent with global data.
Thus, evaluation and management of azoospermia in Bangladesh should integrate clinical
assessment, hormonal markers, imaging, and genetic testing, while applying ASRM, RCOG,
and WHO recommendations within the realities of resource constraints and delayed
presentation.
Infections and Male Infertility :
Recommendation: Strength
Although infections have been linked to male infertility, a direct causal relationship
Strong
has not yet been established [Jung JH,2016].
In cases of male accessory gland infections (MAGI)—particularly prostatitis,
prostatovesiculitis, or prostato-vesiculo-epididymitis—treatment with antibiotics
and nonsteroidal anti-inflammatory drugs (NSAIDs) for 3–6 weeks may be
Weak
| considered. | |
| Following the resolution of infection and inflammation, antioxidant therapy may be used in men with epididymitis to restore the balance of reactive oxygen species (ROS). | Weak |
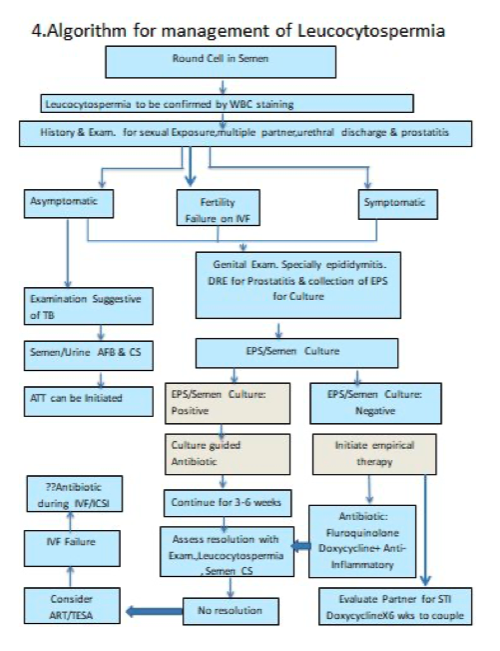
| Empirical use of antibiotics in men with leukocytospermia but without confirmed infection is not recommended, as it has not been shown to improve fertility outcomes. | Strong |
Infections are implicated in male infertility, though a definitive causal link remains unproven.
Infective processes can impair semen quality by inducing oxidative stress, a key mechanism of
sperm damage [Qing L, 2017].
Leukocytospermia (LCS)—defined as >1 × 10⁶ WBCs/mL semen—is not uniformly interpreted
due to variable reference values for peroxidase-positive cells. Accurate distinction between
leukocytes, immature germ cells, and macrophages is crucial. Notably, semen leukocytes are
not a reliable marker of genital tract infection, as they may appear without microbial evidence
[Bezold G, 2007].
Per ASRM and RCOG guidelines, empirical antibiotic therapy for LCS without a detected
pathogen does not improve fertility outcomes. However, when male accessory gland infection
(MAGI)—such as prostatitis, vesiculitis, or epididymitis—is confirmed, antibiotics and anti-
inflammatory agents are warranted.
In Bangladesh, infectious infertility deserves special focus. Genitourinary tuberculosis (GU-TB)
remains a significant, often underdiagnosed cause of azoospermia and obstruction. Early
diagnosis and anti-tubercular therapy are essential to prevent irreversible damage. High rates
of sexually transmitted infections (STIs) further highlight the need for comprehensive
screening.
First-line therapy typically includes fluoroquinolones for 28–42 days, though emerging
resistance necessitates alternatives such as third-generation cephalosporins, trimethoprim,
azithromycin, or doxycycline. Following infection resolution, antioxidant therapy may help
normalize reactive oxygen species (ROS) balance.
Overall, management should combine accurate semen cell differentiation, microbiologic
testing, and pathogen-directed therapy, in alignment with ASRM and RCOG recommendations,
while addressing regional priorities such as GU-TB.
Genetics in male infertility
Genetic Evaluation in Male Infertility
Recommendation: Strength
| In azoospermic men, elevated LH and FSH levels should trigger genetic testing. | Moderate |
| Men with sperm counts <10 million/mL (especially <5 million/mL) due to idiopathic spermatogenic defects should undergo genetic counseling, karyotyping, and Y- chromosome microdeletion testing. | Strong |
| Non-Obstructive Azoospermia (NOA) | |
| Recommendation Strength | |
| Microdissection TESE offers the highest chance of sperm retrieval in men with NOA. | Moderate |
| Klinefelter Syndrome & AZF Deletions | |
| Recommendation Strength | |
| In Klinefelter syndrome, sperm retrieval rates using microdissection TESE range from 22–50%.[ Behre HM,2000] | Moderate |
| Transmission risk of Klinefelter syndrome to offspring is low. | Moderate |
| Young men with AZFc deletions should receive genetic counseling about transmission risks; sperm retrieval rates with microdissection TESE can reach ~55%.[ Okutman O,2018] | Moderate |
| Obstructive Azoospermia & CBAVD | |
| Recommendation Strength | |
| Low-volume ejaculate, acidic pH, and absent fructose suggest obstructive azoospermia, most often due to CBAVD or EDO. | Strong |
| CBAVD accounts for up to 30% of obstructive azoospermia cases. | Moderate |
| CBAVD is diagnosed clinically by the absence of bilateral vasa on palpation. | Strong |
| Genetic evaluation for CBAVD should include testing for CFTR mutations.[ Greco E,2013] | Strong |
| Comprehensive genetic testing of both partners is essential to prevent transmission of genetic disorders to offspring. | Strong |
| Sperm retrieval in CBAVD is successful in up to 97% of cases using testicular or epididymal aspiration. | Weak |
Varicocele, Microlithiasis, and Male Infertility
Varicocele
Recommendation: Only clinically palpable varicoceles require treatment [Baazeem A,2011] Microsurgical varicocelectomy is the preferred surgical method [Ding H,2012] Unconsummated marriage
May result from erectile dysfunction (ED), female factors such as
vaginismus/dyspareunia, or poor knowledge of reproductive anatomy
Perform office sildenafil test to evaluate erectile function If unresponsive to PDE5 inhibitors, consider office intracavernosal injection of
vasoactive drugs (ICIVAD) to assess vasculogenic ED
Men with vasculogenic ED unresponsive to nonsurgical measures should engage in
shared decision-making for penile prosthesis implantation.
Testicular microlithiasis
Associated with abnormal semen parameters, though direct causation is unproven
[Mahafza WS,2016]
Patients should be counseled and taught testicular self-examination Cancer and infertility
Cryopreservation and fertility counseling must be offered in all relevant cases
[Gupta AA,2013]
Orchiectomy should not be delayed for fertility preservation [Trost LW,2012] Risk of hypogonadism should be explained, and baseline hormones assessed Onco-TESE may be considered in rare azoospermia cases with bilateral testicular
tumors [Carrasquillo R,2018]
Cryptorchidism
Testicular biopsy during orchiopexy should be done to rule out malignancy TESE can be considered in cases of azoospermia associated with cryptorchidism Men with unilateral cryptorchidism have paternity rates comparable to those of
individuals without cryptorchidism.
Orchiopexy performed after 6–12 months significantly reduces spermatogenesis Strength
Strong
Strong
(Clinical
Practice)
Weak
Moderate
Strong
–
Moderate
Strong
Moderate
Moderate
Moderate
Moderate
Moderate
Moderatecompared to earlier intervention.
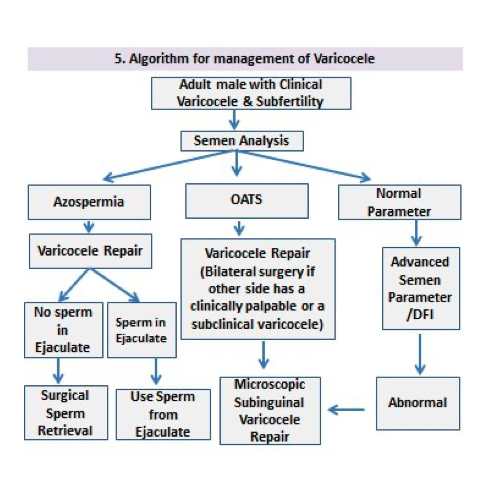
Varicocele is a major contributor to male infertility, linked to testicular hypotrophy and
impaired semen quality [ASRM, 2014]. The diagnostic role of ultrasonography and color
Doppler imaging remains debated, as subclinical varicoceles show poor correlation with
physical findings. Both ASRM and RCOG guidelines note that subclinical varicocele is rarely
clinically significant and repair is not routinely recommended. The Indian (USI, 2021) and
OGSB (2024 draft) guidelines similarly discourage treatment due to limited fertility benefit.
In contrast, surgical varicocelectomy significantly improves semen parameters in men with
palpable varicocele and abnormal semen findings, including selected cases of non-obstructive
azoospermia [Esteves et al., 2016]. Some patients with hypospermatogenesis or late
maturation arrest may regain sperm in the ejaculate post-repair. Across ASRM, RCOG, Indian,
and OGSB guidelines, varicocelectomy is advised when:
A palpable varicocele is present,
The couple has documented infertility,
The female partner’s fertility is normal or treatable, and
The male partner shows abnormal semen parameters.
In Bangladesh, management must consider resource constraints, surgical expertise, and cost.
Physical examination remains the diagnostic mainstay; advanced imaging is used selectively.
Surgical repair is offered primarily in tertiary centers when fertility is a key concern.
Testicular microlithiasis is rare (0.7–6%) and of uncertain clinical significance. Though
associated with malignancy, routine screening is not recommended in asymptomatic men.
Testicular cancer may impair fertility via gonadal damage or gonadotoxic therapy
(chemotherapy, radiotherapy) [53,54]; sperm banking is recommended where possible, though
access remains limited in Bangladesh.
Unconsummated marriage (UCM) is another important but underrecognized cause of male
infertility, representing up to 17% of sexual health clinic visits internationally [55]. In
Bangladesh, it is likely underreported due to stigma and cultural sensitivities, underscoring the
need for structured evaluation and counseling within infertility services.
Idiopathic infertility
Recommendation: Strength
Prior to classifying a male as having unexplained or idiopathic infertility, all other
strong
etiologies should be excluded.[ Hamada A,2012]
There is no established curative treatment for idiopathic or unexplained infertility moderate
Empirical medical therapy (EMT), encompassing hormonal agents and antioxidants,
moderate
may be considered for these patients.[ Attia AM,2013]EMT should be administered initially for a minimum of 4–6 months (approximately
two spermatogenic cycles) before resorting to assisted reproductive technologies
Weak
Patients with an abnormal T/E2 ratio may benefit from a co-treatment with
aromatase inhibitors.
Moderate
30%–80% of infertile men have elevated seminal ROS levels, a potentially treatable
condition
Weak
Oxidation–reduction potential is a better representative for oxidative stress (OS) as
it provides an overall measure of the activity of both oxidants and
Weak
reductants[Tremellen K.,2008]
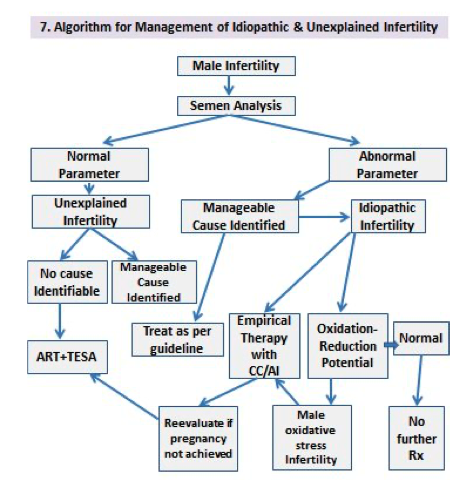
Idiopathic and Unexplained Male Infertility
Unexplained male infertility is diagnosed when semen parameters are normal and both
physical and endocrine evaluations are unremarkable, with no identifiable female factor [56].
In contrast, idiopathic infertility refers to men with abnormal semen parameters but no clear
etiology despite full evaluation.
Before either diagnosis, a comprehensive exclusion of other causes is essential—repeat semen
analysis, infection screening, hormonal assays, genetic tests, and imaging as indicated [Jue JS,
2017].
This approach aligns with ASRM, RCOG, Indian, and OGSB recommendations emphasizing
exhaustive evaluation before labeling a case as idiopathic or unexplained.
Empirical Medical Treatment (EMT)
There is no definitive cure for idiopathic or unexplained male infertility. Management is
empirical and pragmatic, mainly through hormonal therapy or antioxidant regimens to
enhance semen quality and pregnancy rates.
Evidence of benefit remains limited, and couples must be counseled on cost and uncertain
efficacy (ASRM, RCOG).
Indian and OGSB guidelines support selective use of EMT, especially where ART access is
restricted, which applies to many Bangladeshi settings.
Hormonal Therapies
Selective Estrogen Receptor Modulators (SERMs) such as clomiphene citrate may be used in
men with normal testosterone but relative estrogen excess (T/E₂ > 10).
When T/E₂ < 10, aromatase inhibitors (anastrozole, letrozole) can restore androgen–estrogen
balance and support spermatogenesis [Madhukar D, 2009].
ASRM and RCOG recognize these as off-label, empirical options requiring individualized use
and endocrine monitoring, a stance echoed by Indian and OGSB guidance.Antioxidant Therapy
Oxidative stress contributes to sperm dysfunction in up to 30–80% of infertile men.
Measurement of oxidation–reduction potential (ORP) provides an integrated redox
assessment and may outperform isolated ROS assays.
Both ASRM and RCOG endorse antioxidant therapy for men with documented oxidative stress
but caution about limited outcome data.
In Bangladesh, antioxidants are widely used due to low cost and availability, but clinicians
should document baseline testing and monitor response.
Treatment Duration
When EMT is initiated, a 4–6-month trial (≈ two spermatogenic cycles) is advised before
advancing to ART [Kumar R, 2007].
ASRM and RCOG classify this as a moderate-strength recommendation due to limited
evidence.
In the Bangladeshi context, a defined EMT trial remains practical where ART access is limited,
provided couples are counseled on expected timelines and realistic success rates.
Conclusion
Male factors contribute to nearly half of all infertility cases worldwide. Every infertile couple
should therefore include a urological evaluation of the male partner (ASRM, RCOG, OGSB,
USI/ISAR). The WHO 6th Edition Manual stresses that semen analysis alone cannot define
fertility; results must be interpreted by decision limits to guide management—an important
shift for Bangladesh, where borderline results are often misread.
Treatable causes include hormonal and infectious conditions such as hypogonadotropic
hypogonadism and genital tract infections, while varicocele and obstructive azoospermia are
primarily surgical. Global guidelines endorse microsurgical varicocelectomy for clinical
varicoceles and reconstructive or sperm retrieval procedures where feasible. In Bangladesh,
careful patient selection is essential given limited surgical resources.
Idiopathic infertility, accounting for about one-third of cases, has limited response to empirical
therapies (hormones, antioxidants). ASRM and RCOG recommend cautious, time-limited use
only after excluding other causes, while OGSB advises restricting such therapy before
considering ART. In Bangladesh, where ART access is limited, clinicians must emphasize realistic
counselling.
Cultural and financial factors also shape care. In Bangladesh and India, donor insemination and
adoption remain vital alternatives when medical or surgical options fail. Early counselling on
these options helps reduce psychological distress and delay.In essence, male infertility management must be evidence-based, individualized, and context-
aware. Adapting international standards (ASRM, RCOG, OGSB, Indian guidance) to local
realities—through cost-sensitive, research-informed approaches—offers the most practical
path forward.
Conflicts of Interest: There are no conflicts of interest.
Male Infertility Algorithm
APPENDICES
| System/Region | Key Examination Findings |
| General | • Overweight/obesity may impair spermatogenesis. • Assess virilization for pubertal development and androgen status. • Gynecomastia may indicate endocrine disorders. |
| Abdomen | • Look for scars from previous pelvic or urogenital surgeries that may affect fertility. |
| Phallus | • Check meatal location; hypospadias/epispadias can hinder semen deposition. • Palpate for plaques (e.g., Peyronie’s disease) that may make intercourse difficult. • Identify lesions, ulcers, or discharge suggesting a sexually transmitted infection. |
| Scrotum & Testes | • Note scars from prior scrotal surgery/trauma. • Confirm testicular location in scrotum (vital for function). • Assess size, consistency, and contour (spermatogenesis- related); look for masses suspicious of testicular cancer. |
| Epididymides | • Evaluate shape and consistency for normal development. • Induration/dilatation may indicate obstruction. • Epididymal cysts or spermatoceles may also contribute to obstruction. |
| Vas Deferens | • Confirm continuity and contour; agenesis may suggest CFTR mutation or Wolffian duct abnormality. • Identify vasectomy-related defects or granulomas. |
| Digital Rectal Examination (DRE) | • Look for midline prostatic cysts or dilated seminal vesicles, which may indicate ejaculatory duct obstruction (EDO). |
Appendix I: Male Reproductive Health Physical Examination
The purpose of the physical examination is to detect possible causes of reproductive problems,
underlying health conditions, or modifiable factors that may enhance overall health and fertility
outcomes.
ABBREVIATIONS
| ABVD | Adriamycin, Bleomycin, Vinblastine, and Dacarbazine |
| ACOG | American College of Obstetricians and Gynecologists |
| AMA | American Medical Association |
| ASCO | American Society of Clinical Oncology |
| ASRM | American Society for Reproductive Medicine |
| AUA | American Urological Association |
| AUAER | American Urological Association Education and Research, Inc. |
| ASA | Antisperm Antibody |
| AIs | Aromatase Inhibitors |
| ART | Assisted Reproductive Technology |
| AZF | Azoospermia Factor |
| BOD | Board of Directors |
| BPA | Bisphenol A |
| CVD | Cardiovascular Disease |
| CCI | Charlson Comorbidity Index |
CBAVD Congenital Bilateral Absence of the Vas Deferens
CF Cystic Fibrosis
CFTR Cystic Fibrosis Transmembrane Conductance Regulator
DNA Deoxyribonucleic acid
DFI DNA Fragmentation Index
DEHP Di-2-ethylhexyl phthalate
EDO Ejaculatory Duct Obstruction
ECRI Emergency Care Research Institute
FOE Failure of Emission
FSH Follicle-Stimulating Hormone
hCG Human Chorionic Gonadotropin
HH Hypogonadotropic Hypogonadism
IB Immunobead
IVF In Vitro Fertilization
ICSI Intracytoplasmic Sperm Injection
IUI Intrauterine Insemination
LRL Lower Reference Limits
LH Luteinizing Hormonemicro-TESE Microdissection-Testicular Sperm Extraction
MRI Magnetic Resonance Imaging
NOA Non‐Obstructive Azoospermia
OR Odds Ratio
PGC Practice Guidelines Committee
RCTs Randomized Controlled Trials
RPL Recurrent Pregnancy Loss
RR Relative Risk
RE Retrograde Ejaculation
RPLND Retroperitoneal Lymph Node Dissection
ROB Risk of Bias
SQC Science and Quality Council
SERMs Selective Estrogen Receptor Modulators
SA Semen Analysis
SRR Sperm Retrieval Rates
TL Telomere
TESE Testicular Sperm Extraction
TRUS Transrectal UltrasonographyTURED WHO Transurethral Resection of Ejaculatory Ducts
World Health Organization
Compiled By
Dr. Fahmida Rashid
Dr. Rubina Akhter
Compiled By
1. Prof Fawzia Hossain
2. Dr Ummul Warda
3. Dr Amena Fardous
4. Dr Tanzia Akhter
5. Dr Maniza Khan
6. Dr Ananna Zakia
7. Dr Lutfa Amin
8. Dr Tasrina Akhter
9. Dr Amrita Saha
10. Dr Tasnuva Maliha
