

Background
Shoulder dystocia is defined as a vaginal cephalic delivery that requires additional obstetric manoeuvres to deliver the fetus after the head has delivered and gentle traction has failed.
Shoulder dystocia occurs when either the anterior, or less commonly the posterior, fetal shoulder impacts on the maternal symphysis, or sacral promontory, respectively.
Incidences between 0.58% and 0.70%.
Maternal morbidity includes postpartum haemorrhage (11%) and third and fourth-degree perineal tears (3.8%).
Brachial plexus injury (BPI) is one of the most important fetal complications of shoulder dystocia, fewer than 10% resulting in permanent neurological dysfunction.
Purpose and scope
Prediction, prevention and management of shoulder dystocia; it does not cover primary prevention of fetal macrosomia associated with gestational diabetes.
Prediction
Clinicians should be aware of existing risk factors in labouring women and must always be alert to the possibility of shoulder dystocia.
Risk assessments for the prediction of shoulder dystocia are insufficiently predictive to allow prevention of the large majority of cases.
Infants of diabetic mothers have a two- to four-fold increased risk of shoulder dystocia compared with infants of the same birth weight born to non-diabetic mothers.
Prevention of Shoulder Dystocia
Induction of labour does not prevent shoulder dystocia in non-diabetic women with a suspected macrosomic fetus.
Induction of labour at term can reduce the incidence of shoulder dystocia in women with gestational diabetes.
Elective caesarean section should be considered to reduce the potential morbidity for pregnancies complicated by pre-existing or gestational diabetes, regardless of treatment, with an estimated fetal weight of greater than 4-5 kg.
Either caesarean section or vaginal delivery can be appropriated after a previous shoulder dystocia. The decision should be made jointly by the woman and her carers.
Recurrence rate of shoulder dystocia of between 1% and 25%.
There is no requirement to recommend elective caesarean birth routinely.
Management of Shoulder Dystocia
All birth attendants should be aware of the methods for diagnosing shoulder dystocia and the techniques required to facilitate delivery.
Birth attendants should routinely look for the signs of shoulder dystocia.
Timely management of shoulder dystocia requires prompt recognition. The attendant health carer should routinely observe for:
- Difficulty with delivery of the face and chin
- The head remain tightly applied to the vulva or even retracting (turtle-neck sign)
- Failure of restitution of the fetal head
- Failure of the shoulders to descend
Routine traction in an axial direction can be used to diagnose shoulder dystocia but any other traction should be avoided.
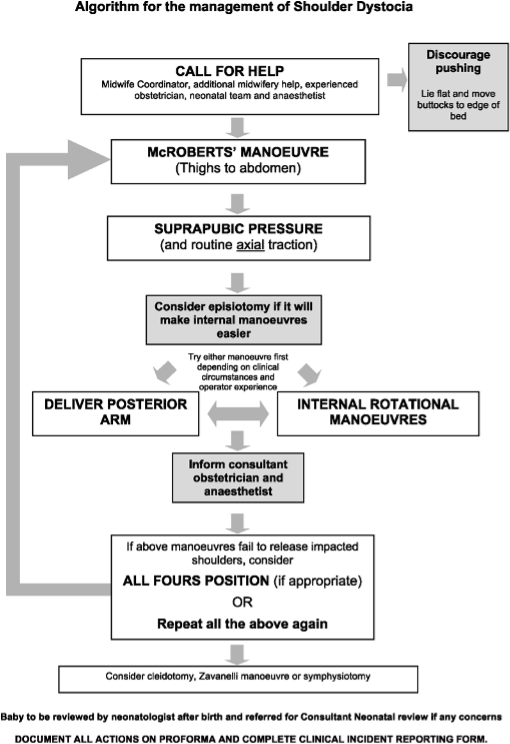
Shoulder dystocia should be managed systematically.
Immediately after recognition of shoulder dystocia, additional help should be called.
The problem should be stated clearly as ‘this is shoulder dystocia’ to the arriving team.
Fundal pressure should not be used.
McRoberts’ manoeuvre is a simple, rapid and effective intervention and should be performed first.
Suprapubic pressure should be used to improve the effectiveness of the McRoberts’ manoeuvre.
An episiotomy is not always necessary.
Internal manoeuvres or ‘all-fours’ position should be used if the McRoberts’ manoeuvre and suprapubic pressure fail.
All-fours technique: success 83%.
Third-line manoeuvres should be considered very carefully to avoid unnecessary maternal morbidity and mortality, particularly by inexperienced practitioners.
Birth attendants should be alert to the possibility of postpartum haemorrhage and severe perineal tears.
The baby should be examined for injury by a neonatal clinician.
An explanation of the delivery should be given to the parents.
Risk Management
All maternity staff should participate in shoulder dystocia training at least annually.
Compiled By:
Dr. Nibadita Ghosh
Contributors :
1. Prof Fawzia Hossain
2. Prof Shaheen F Rahman
3. Dr Sumaiya Binte Asif
4. Dr Taslima Tithi
5. Dr Maniza Khan
6. Dr Sohelee Nargis
7. Dr Tahera Fatima
8. Dr Arunthiya Soma Saha
9. Dr Nayer Islam
10. Dr Rafaa Islam
11. Dr Sayema Tabassum
