

Prepared by :
Dr Farhana Khatoon,
Associate Professor,
Gynaecological Oncology, BMU
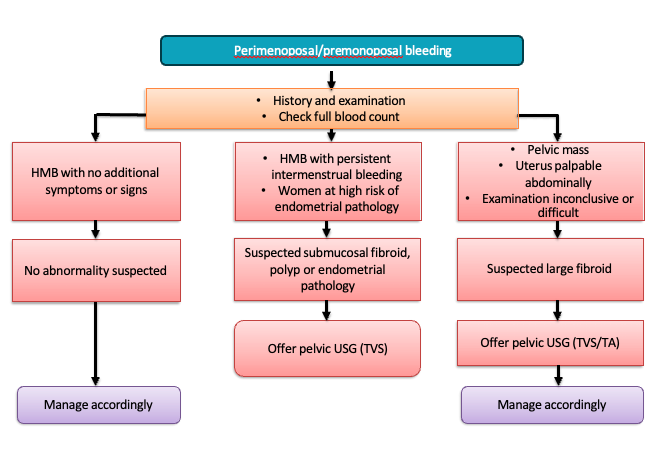
Evaluation of Pre and Perimenopausal Bleeding
History:
- Abnormal vaginal bleeding is the most common symptom.
- Premenopausal women with abnormal uterine bleeding, particularly if there is a history of anovulation, infertility, or PCOD.
- Perimenopausal patients with intermenstrual bleeding or increasingly heavy periods.
- Women from families with Lynch Syndrome.
- History of unopposed estrogen therapy or tamoxifen therapy.
Medical History (MH):
- DM, HTN, thyroid disorder, aspirin, OCP.
General Examination (G/E):
- Anaemia, weight, breast, BP, BMI.
Per Abdominal Examination (P/A):
- Normal findings, mass in abdomen.
Per Speculum Examination (P/S):
- Cervix: Any growth, polyp, or discharge.
Bimanual Examination (B/M):
- Uterus: Size, position, and shape.
Rectovaginal Examination (R/V/E):
- Evaluation of ovaries, fallopian tube, POD, parametrium.
Approach based on findings:
Management of Postmenopausal Bleeding & Endometrial Carcinoma
Introduction:
- Any bleeding or spotting after 12 months of no periods is considered postmenopausal bleeding and requires prompt evaluation by an Ob-Gyn.
- Incidence: ~10% of PMB cases are endometrial cancer.
- Red flag symptom – requires prompt evaluation by an Ob-Gyn.
- Guidelines stress early detection, risk stratification, MDT care.
Risk Factors for Endometrial Cancer:
- Unopposed estrogen exposure (HRT, PCOS, obesity)
- Tamoxifen therapy
- Lynch syndrome (HNPCC)
- Nulliparity, late menopause
- Diabetes, hypertension, metabolic syndrome
Evaluation of Postmenopausal Bleeding (PMB):
- History of bleeding pattern and risk factors assessment (e.g., Tamoxifen use, obesity, family history).
- Examination: general, pelvic, speculum, bimanual (to exclude atrophic changes, polyp, visible growth)
- First-line investigation:
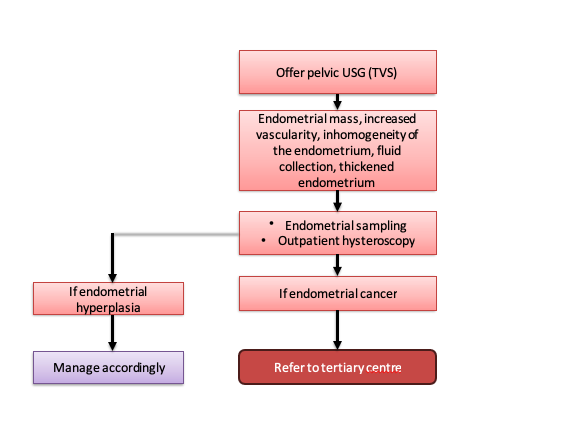
Transvaginal Ultrasound (TVS):
- Endometrium ≤4 mm → Very low risk of cancer → Reassure (if no persistent/recurrent bleeding).
- Endometrium >4 mm OR endometrium not well-visualized → Proceed to Endometrial Biopsy.
Endometrial Biopsy:
- Benign / Atrophy → Reassure.
- Hyperplasia / Carcinoma → Manage accordingly (refer to oncology/appropriate treatment).
- Persistent or Recurrent Bleeding (even with thin endometrium or benign biopsy) → Hysteroscopy ± D&C (to rule out focal lesion, polyps, type II carcinoma).
- Tamoxifen users: Higher risk → Consider direct biopsy or hysteroscopy even if endometrium thin.
- High-risk women (obesity, Lynch syndrome, strong FH): Lower threshold for biopsy.
Summary:
- TVS first for low-risk women.
- Biopsy if thickened endometrium, inconclusive TVS, or risk factors.
- Hysteroscopy if recurrent/persistent bleeding or inconclusive results.
Patient Presenting with Biopsy-Proven Endometrial Carcinoma
Primary Level: Early detection and referral.
Secondary Level:
Additional History:
- Women from families with Lynch Syndrome.
- History of unopposed estrogen therapy or tamoxifen therapy.
- Pelvic/abdominal pain
- Urinary frequency / urgency
Physical Examination:
- General examination: Anaemia, edema, weight loss, breast, lymph nodes (especially supraclavicular and inguinal LN)
- Per abdominal examination: Usually normal findings; mass in abdomen (mass in uterus, pyometra, haematometra, synchronous adnexal mass); Ascites
- Per Speculum Examination (P/S): Cervix: Any growth, polyp, or discharge
- Bimanual Examination (B/M): Uterus: Size
- R/V/E: Evaluation of ovaries, fallopian tube, POD, parametrium
Investigations:
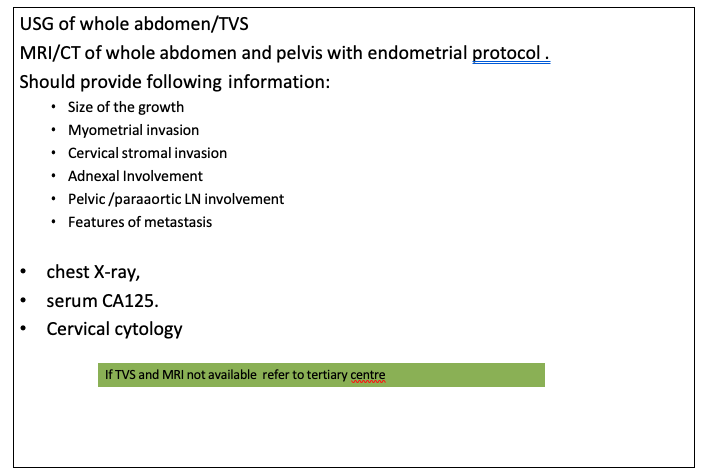
Tertiary Level:
- Pre-op workup: MRI/CT with protocol, chest X-ray, serum CA125
- Multidisciplinary team (MDT) involvement
- If diagnostic dilemma → Immunohistochemistry for clarity
- Depending on clinical and pathologic risk, additional imaging modalities (thoracic, abdominal and pelvic CT scan, MRI, PET scan, or ultrasound) should be considered to assess ovarian, nodal, peritoneal, and other sites of metastatic disease
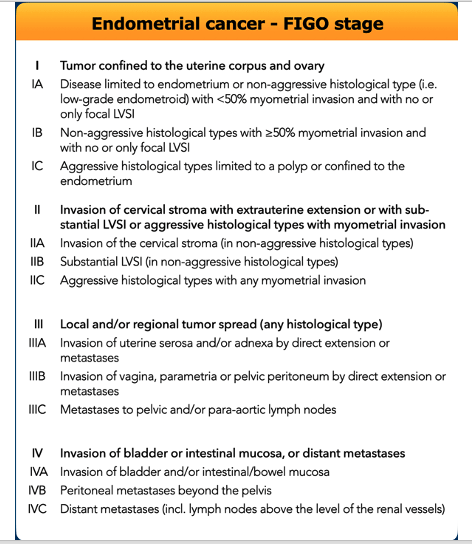
Reference: Concin N, et al. Int J Gynecol Cancer 2021;31:12–39. doi:10.1136/ijgc-2020-002230
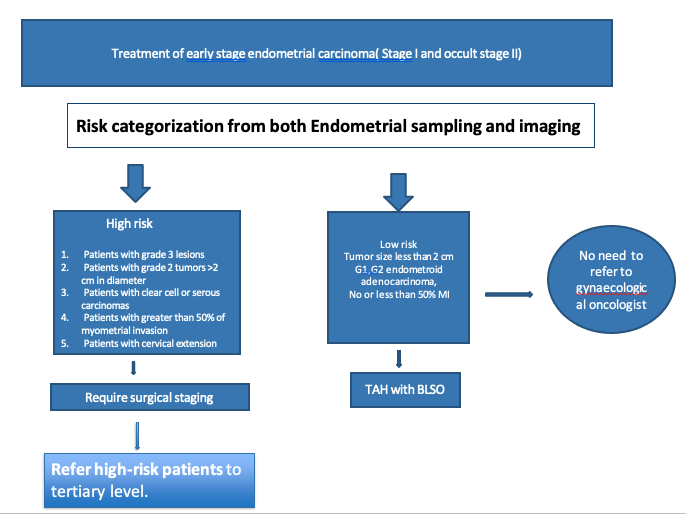
Management
Risk Categorization:
- Low Risk: Tumor size <2 cm; G1, G2 endometrioid adenocarcinoma; No or <50% myometrial invasion
- High Risk: Grade 3 lesions; Grade 2 tumors >2 cm; Clear cell or serous carcinomas, non-endometrioid variety; ≥50% myometrial invasion; Cervical extension
ESGO/ESTRO/ESP Guidelines:
- Planning of staging and treatment should be on MDT basis
- Patients should be carefully counseled
- Treatment should be undertaken in a specialized center by dedicated specialists
Early Stage Disease:
- Minimally invasive surgery preferred
- Avoid intra-peritoneal tumor spillage, rupture, morcellation
- Standard surgery: total hysterectomy + bilateral salpingo-oophorectomy without vaginal cuff resection
- Staging infracolic omentectomy in stage I serous, carcinosarcoma, undifferentiated carcinoma
- Sentinel lymph node biopsy for low/intermediate-risk
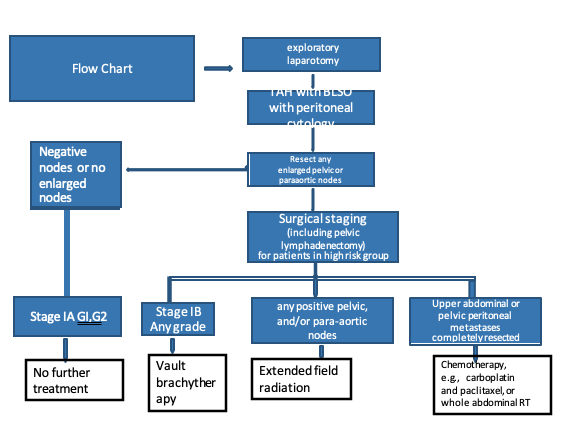
High-Risk EC:
- Lymphadenectomy ± omentectomy
- Lower midline laparotomy, peritoneal washings, exploration, excision of suspicious lesions
- Para-aortic LN dissection if grossly positive pelvic nodes, positive adnexae, grade 2/3 with outer-third MI
Medically Unfit Patients:
- Vaginal hysterectomy ± BSO if feasible
- Definitive radiotherapy: EBRT + brachytherapy for high-grade/deep MI; brachytherapy alone for low-grade
- Systemic treatment if unsuitable for surgery/radiotherapy
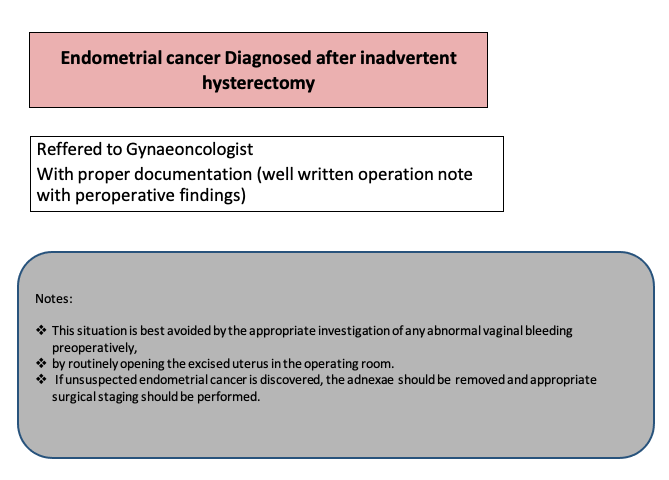
Do’s:
- Midline incision, remove tubes & ovaries, assess tumor size, MI, cervical extension, appropriate staging, HPE in tertiary center
Don’ts:
- Don’t preserve any ovary if TAH is performed
Notes:
- Low-risk EC can be approached laparoscopically
- High-risk EC should be managed by gynae-oncologist in tertiary care center
- Referral should include biopsy findings, slides, and blocks
Molecular Markers
- Markers: p53, MSH6, PMS2, POLE mutation
- Molecular classification encouraged, especially in high-grade tumors
- POLE mutation may be omitted in low/intermediate-risk, low-grade histology
Prognostic Groups:
- POLEmut → excellent prognosis
- p53-abn → poor prognosis
- MMRd or NSMP → intermediate prognosis
Adjuvant Treatment:
- Low-risk (stage IA, G1, G2) → no adjuvant treatment
- Intermediate risk → brachytherapy recommended to decrease vaginal recurrence
- High intermediate risk → brachytherapy, EBRT ± chemotherapy depending on grade, LVSI
- High-risk (stage III–IVA, non-endometrioid, myometrial invasion) → EBRT + chemo or sequential therapy
- Advanced disease → surgical tumor debulking if feasible, systemic therapy, MDT & palliative care
Chemotherapy: Carboplatin + paclitaxel
Immunotherapy: Pembrolizumab + lenvatinib (dMMR/MSI-H)I
Radiotherapy: recurrence/palliation
MDT & palliative care
Ref: NCCN 2025; ESMO 2023
Endometrial Cancer in Young / Pre-Menopausal Women
Fertility-Sparing Eligibility:
- Age <40 years
- Desire for fertility
- G1 Endometrioid histology
- No myometrial invasion (MRI/TVS)
- No cervical/adnexal/LVSI involvement
Fertility-Sparing Therapy:
- Medroxyprogesterone acetate 400–600 mg/day
- Megestrol acetate 160–320 mg/day
- Optional: LNG-IUS
- Biopsy & imaging every 3–6 months
Follow-Up
| Time Since Treatment | Frequency | What to Assess |
|---|---|---|
| First 2 years | Every 3–6 months | History, pelvic exam, vault exam, symptoms |
| Years 3–5 | Every 6–12 months | Same as above |
| After 5 years | Annually | General health surveillance |
| Imaging / Labs | Only if symptoms or suspicion of recurrence | – |
| Vaginal vault cytology | Optional | Not routine in asymptomatic patients |
Key Updates (RCOG vs Old Protocols)
- TVS cutoff = 4 mm for PMB
- Sentinel node mapping preferred
- Molecular classification (POLE, MMRd, p53)
- Broader fertility-sparing management
Summary:
- PMB must always be investigated
- ET cutoff = 4 mm
- Risk- & molecular-based management standard
- MDT care essential
References:
- RCOG Green-top Guideline 67 (2022)
- ESGO/ESTRO/ESP Endometrial Cancer Guideline (2021)
- NCCN Uterine Neoplasms v1.2025
- ESMO Clinical Practice Guideline: Endometrial Cancer (2023)
Ref: RCOG GTG 67; NCCN 2025
Compiled By
Dr Farhana Khatoon,
Contributors
1. Prof Dr Fawzia Hossain
2. Dr Tasnuva Akhter
3. Dr Maniza Khan
4. Dr Nurun Nahar
5. Dr Ananna Zakia
6. Dr Lutfa Amin
7. Dr Tasrina Akhter
8. Dr Amrita Saha
9. Dr Lutfa Akhter
10. Dr Aklima Zakaria Zinan
