

Genetic screening
Used when number of particular population are offered a test for a condition or carrier status when there is no prior evidence of its presence in an individual.
Genetic testing
Is the analysis of DNA, RNA, Chromosome, protein or metabolites in order to detect alteration related to heritable disorders.
Definition of Congenital anomaly
Congenital anomalies are also known as birth defects, congenital disorders or congenital malformations. Congenital anomalies can be defined as structural or functional anomalies (for example, metabolic disorders) that occur during intrauterine life and can be identified prenatally, at birth, or sometimes may only be detected later in infancy.
Incidence
An estimated 240,000 newborns die worldwide within 28 days of birth every year due to congenital disorders. Congenital disorders cause a further 170,000 deaths of children between the ages of 1 month and 5 years.
Structural abnormalities occur in approximately 3% of live births, and congenital abnormalities account for 20–25% of perinatal death.
In Bangladesh incidence was found from 2.54% to 4.42% in different studies.
The most common severe congenital disorders are heart defects, neural tube defects and Down syndrome.
Classification of anomaly
Primarily structural
- Genetic
- Other
Primarily metabolic
- Mostly genetic
The goal of screening
To provide individuals with information that will permit them to make informed reproductive decisions.
Steps of screening
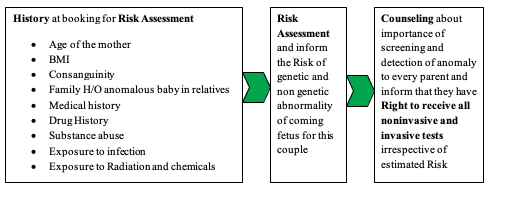
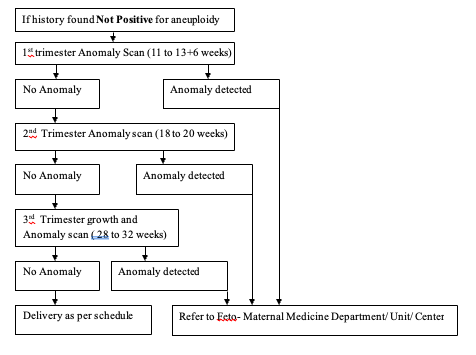
Screening of Low Risk patients
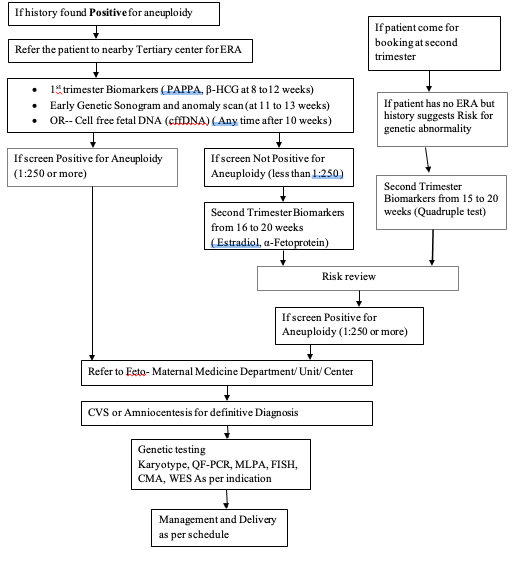
Screening of High Risk patients
Fetal Echocardiogram
Time of Fetal Echocardiogram: Should preferably perform between 18 to 22 weeks.
Indication of Fetal Echocardiogram
Fetal Factors
- Suspected cardiac structural anomaly
- Suspected abnormality in cardiac function
- Hydrops fetalis
- Persistent fetal tachycardia (heart rate > 180 beats per minute)
- Persistent fetal bradycardia (heart rate < 120 beats per minute) or a suspected heart block
- Frequent episodes or a persistently irregular cardiac rhythm
- Major fetal extracardiac anomaly
- Nuchal translucency of 3.0 mm or greater or at or above the 99th percentile for gestational age
- Chromosomal abnormality by invasive genetic testing or with cell-free fetal DNA screening
- Monochorionic twinning
- Systemic venous anomaly (e.g., a persistent right umbilical vein, left superior vena cava, or absent ductus venosus)
Maternal or Familial Disease or Maternal Environmental Exposure
- Pregestational diabetes regardless of the hemoglobin A1C level
- Gestational diabetes diagnosed in the first or early second trimester
- In vitro fertilization, including intracytoplasmic sperm injection
- Phenylketonuria (unknown status or a periconceptional phenylalanine level > 10 mg/dL)
- Autoimmune disease with anti-Sjögren syndrome–related antigen A antibodies and with a prior affected fetus
- First-degree relative of a fetus with CHD (parents, siblings, or prior pregnancy)
- First- or second-degree relative with disease of Mendelian inheritance and a history of childhood cardiac manifestations
- Retinoid exposure or selected teratogen exposure (e.g., paroxetine, carbamazepine, or lithium)
- First-trimester rubella infection
- Antihypertensive medication limited to angiotensin-converting enzyme inhibitors
- Second-degree relative of a fetus with CHD
Other Considerations
A detailed fetal anatomic ultrasound examination which includes an evaluation of the fetal heart may be appropriate instead, with fetal echocardiography performed only if an abnormality is suspected.
- Obesity (body mass index ≥30 kg/m²)
- Selective serotonin reuptake inhibitor antidepressant exposure other than paroxetine
- Noncardiac “soft marker” for aneuploidy in the absence of karyotype information
- Abnormal maternal serum analytes (e.g., α-fetoprotein level)
- Isolated single umbilical artery
- Warfarin exposure and alcohol exposure
- Echogenic intracardiac focus in anomaly scan
- Maternal fever or viral infection with seroconversion only
- Isolated CHD in a relative further removed from second degree to the fetus
Reference
World Health Organization Fact sheet on Congenital Disorders. 27 February 2023. https://www.who.int/news-room/fact-sheets/detail/birth-defects
Teresa Marino, Ronald M Ramus. Prenatal Diagnosis for Congenital Malformations and Genetic Disorders. Feb 17, 2021. https://emedicine.medscape.com/article/1200683-overview?form=fpf
Podder, R., Zeba, D., Fatema, K., Alam, S., & Bilkis, R. Prevalence, Pattern and Outcome of Congenital Anomalies in Patients Admitted at a Tertiary Level Hospital in Bangladesh. Bangabandhu Sheikh Mujib Medical College Journal, 2024. 3(1): 27–31. https://doi.org/10.3329/bsmmcj.v3i1.71956
Sultana MT, et al. Types and Distribution of Fetal Congenital Anomaly and their Maternal Characteristics in High Risk Pregnancy Unit of Dhaka Medical College Hospital, Bangladesh. J Gynecol 2022, 7(1): 000229. https://doi.10.23880/oajg-16000229
De Robertis V, Calì G, et al. Corbella et al.; Italian society of ultrasound in Obstetrics and Gynecology (SIEOG) working group on the obstetric referral scan. Referral scan for congenital anomalies: time to agree on indications. Ultrasound Obstet Gynecol. 2022; 60(5): 597–603. https://doi.org/10.1002/uog.24950
American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics; Committee on Genetics; Society for Maternal-Fetal Medicine. Screening for Fetal Chromosomal Abnormalities: ACOG Practice Bulletin, Number 226. Obstet Gynecol. 2020 Oct;136(4):e48–e69. https://doi.10.1097/AOG.0000000000004084
Minnella GP, Crupano FM, Syngelaki A, Zidere V, Akolekar R, Nicolaides KH. Diagnosis of major heart defects by routine first-trimester ultrasound examination: association with increased nuchal translucency, tricuspid regurgitation and abnormal flow in ductus venosus. Ultrasound Obstet Gynecol. 2020; 55(5): 637–644. https://doi.org/10.1002/uog.21956
Salomon LJ, Alfirevic Z, Bilardo CM, et al. ISUOG practice guidelines: performance of first-trimester fetal ultrasound scan. Ultrasound Obstet Gynecol. 2013; 41: 102–113. https://doi.10.1002/uog.12342
Salomon LJ, Alfirevic Z, Berghella V, et al. ISUOG Practice Guidelines (updated): performance of the routine mid-trimester fetal ultrasound scan. Ultrasound Obstet Gynecol. 2022; 59(6): 840–856. https://doi.org/10.1002/uog.24888
AIUM practice parameter for the performance of fetal echocardiography. J Ultrasound Med. 2020; 39: E5–E16. DOI: 10.1002/jum.15188
Compiled By:
Dr. Arifa Sharmin
Contributors :
- Prof Fawzia Hossain
- Dr Shahana Pervin
- Dr Sharmin Salam
- Dr Sumaiya Binte Asif
- Dr Taslima Akter
- Dr Maniza Khan
- Dr Nusrat Adila
- Dr Jerin Tasnim
- Dr Sharmin Alam
- Dr Sajid Bin Ashraf Sami
