

Service organization
* Commissioners and providers, including networks of providers, should ensure that all 4 birth settings (home, freestanding midwifery unit, alongside midwifery unit and obstetric unit) are available to all women (in the local area or in a neighbouring area). [2014, amended 2023)
* Ensure that all women giving birth have timely access to an obstetric unit if they need transfer of care for medical reasons or because they request regional analgesia. Audit and publish transfer times and reasons for delay in transfers so women can be informed of local service availability. [2014. amended 2023]
* Commissioners and providers, including networks of providers, should ensure that there are:
robust protocols in place for transfer of care between settings clear local pathways for the continued care of women who are
transferred from one setting to another, including: o when crossing provider boundaries
* if the nearest obstetric or neonatal unit is closed to admissions or the local midwifery-led unit is full. (2014]
* Commissioners and providers, including networks of providers, should ensure that there are multidisciplinary clinical governance structures in place to enable the oversight of all birth settings. These structures should include, as a minimum, midwifery, obstetric, anaesthetic and neonatal expertise, and adequately supported user representation. [2014 amended 2023J
Planning place of birth
* All women at low risk of complications
* Explain to both multiparous and nulliparous women who are at low risk of complications that giving birth is generally very safe for both the woman and her baby .2014
Advise women that additional resources to help them plan their place of birth are available on the tools and resources page for this guideline and the NHS website. (2023]
* Explain to both multiparous and nulliparous women that they may choose any birth setting (home, freestanding midwifery unit, alongside midwifery unit or obstetric unit), and support them in their choice of setting wherever they choose to give birth:
Advise low risk multiparous women that planning to give birth at home or in a midwifery-led unit (freestanding or alongside) is associated with a lower rate of interventions and the outcome for the baby is no different compared with an obstetric unit.
Advise low-risk nulliparous women that planning to give birth in a midwiferyled unit (freestanding or alongside) is associated with a lower rate of interventions and the outcome for the baby is no different compared with an obstetric unit. Explain that if they plan birth at home, there is a small increase in the risk of an adverse outcome for the baby. [2014, amended 2023]
* Ensure that all”healthcare professionals involved in the care of pregnant women are familiar with the types and frequencies of serious medical problems that can affect babies in order to be able to provide this information to women if they request it. (2014]
* Discuss with women the following information, including local statistics, about all local birth settings, and update them if this changes during their pregnancy:
access to midwives, including:
* the likelihood of being cared for in labour by a familiar midwife
* the likelihood of receiving one-to-one care throughout labour (not necessarily being cared for by the same midwife for the whole of labour)
access to medical staff (obstetric, anaesthetic and neonatal) availability of birthing pools
access to pain relief, including Entonox (a 50:50 mixture of oxygen and nitrous oxide) and medicines (for example, pethidine, diamorphine, patientcontrolled analgesia and regional analgesia)
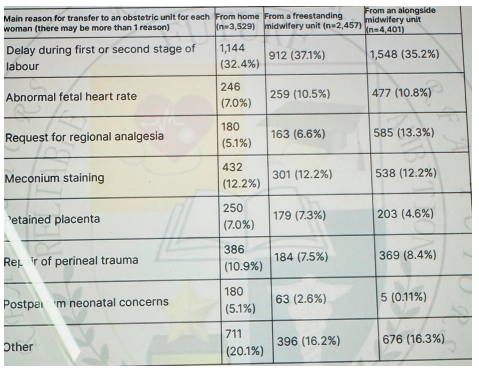
the likelihood of being transferred to an obstetric unit (if this is not the woman’s chosen place of birth), the reasons why this might happen, the time it may take, the delay in obstetric or neonatal care this may cause, and how her birth companion will travel; refer to table 1 if no local data is available.
Table 1 Primary reasons for transfer to an obstetric unit by number of women transferred (% of total transferred from each setting)
Impact of BMI on choice of place of birth
* Advise vomen that, in general, the higher their body mass index (BMI) at booking (and particularly with a BMI above 35 kg/m2 ), the greater the likelihood of complications, so this may be something they wish to think about when planning their place of birth. Discuss with them that:
these complications include unplanned caesarean birth postpartum haemorrhage, transfer from home to an obstetric unit, stillbirth, neonatal death or the baby needing neonatal care
the risk of complications may depend on whether the woman is nulliparous or multiparous, but in general the risks of complications are higher for nulliparous women with an increased BMI compared with multiparous women with an increased BMI
in the event of complications arising, advanced care can generally be given more quickly in an obstetric unit or an alongside midwifery unit than at home or in a freestanding midwifery unit
Low-risk multiparous women
* Using tables 2 and 3, explain to low-risk multiparous women that:
planning birth at home or in a freestanding midwifery unit is associated with a higher rate of spontaneous vaginal birth than planning birth in an alongside midwifery unit, and these 3 settings are associated with higher rates of spontaneous vaginal birth than planning birth in an obstetric unit
planning birth in an obstetric unit is associated with a higher rate of interventions, such as vaginal birth with forceps or ventouse, unplanned caesarean birth and episiotomy, compared with planning birth in other settings
there are no differences in outcomes for the baby associated with planning birth in any setting. [2014, amended 2023]
Table 2 Low-risk multiparous women: Rates of different modes of birth, transfer to an obstetric unit and obstetric interventions for each planned place of birth (number of incidences per 1,000 women giving birth by location)
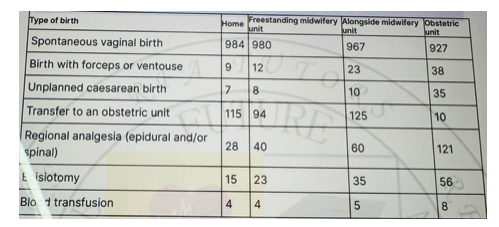
* For obstetric unit transfer to an obstetric unit, the 10 cases noted in table 2 are the estimated transfer rate from one obstetric unit to a different obstetric unit owing to lack of capacity or expertise. For regional anesthesia, Blix et al. reported epidural analgesia and the Birthplace in England study reported spinal or epidural analgesia.
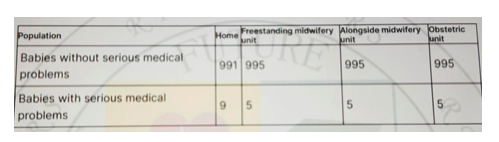
Table Low-risk multiparous women: Outcomes for the baby for each planned place of birth (by number of babies per 1,000 births)
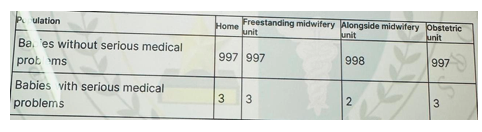
* Serious medical problems were combined in table 3: neonatal encephalopathy and meconium aspiration syndrome were the most common adverse events, together accounting for 75% of the total.
Stillbirths after the start of care in labour and death of the baby in the first week of life accounted for 13% of the events. Fractured humerus and clavicle were uncommon outcomes (less than 4% of adverse events).
Low-risk nulliparous women
* Using tables 4 and 5, explain to low-risk nulliparous women that: planning birth at home or in a freestanding midwifery unit is associated with a higher rate of spontaneous vaginal birth than planning birth in an alongside midwifery unit, and these 3 settings are associated with higher rates of spontaneous vaginal birth than planning birth in an obstetric unit
planning birth in an obstetric unit is associated with a higher rate of interventions, such as vaginal birth with forceps or ventouse, planned caesarean birth and episiotomy, compared with planning birth in other settings
there are no differences in outcomes for the baby associated with planning birth in an alongside midwifery unit, a freestanding midwifery unit or an obstetric unit
planning birth at home is associated with an overall small increase in the risk of a baby having a serious medical problem (about 4 more per 1,000 births) compared with planning birth in other settings.
[2014, amended 2023,
Table 4 Low-risk nulliparous women: Rates of different modes of birth, transfer to an obstetric unit and obstetric interventions for each planned place of birth (number of incidences per 1,000 women giving birth by location)
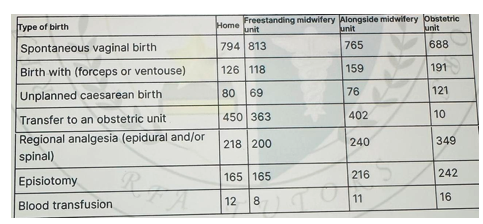
* For obstetric unit transfer to an obstetric unit, the 10 cases noted in table 4 are the estimated transfer rate from one obstetric unit to a different obstetric unit owing to lack of capacity or expertise. For regional anaesthesia, Blix et al. reported epidural analgesia and the Birthplace in England study reported spinal or epidural analgesia.
Table 5 Low-risk nulliparous women: Outcomes for the baby for each planned place of birth (by number of babies per 1,000 births)
* Serious medical problems were combined in table 5: neonatal encephalopathy and meconium aspiration syndrome were the most common adverse events, together accounting for 75% of the total.
Stillbirths after the start of care in labour and death of the baby in the first week of life accounted for 13% of the events. Fractured humerus and clavicle were uncommon outcomes (less than 4% of adverse events).
Medical conditions and other factors that may affect planned place of birth
* Use tables 6 to 9 as part of an assessment for a woman choosing her planned place of birth:
tables 6 and 7 show medical conditions or other situations in which there is increased risk for the woman or baby during or shortly after labour, where care in an obstetric unit would be expected to reduce this risk
the factors listed in tables 8 and 9 are not reasons in themselves for advising birth within an obstetric unit, but indicate that further consideration of birth setting may be needed
discuss these risks and the additional care that can be provided in the obstetric unit with the woman so that she can make an informed choice about the planned place of birth. [2007, amended 2014
Table 6 Medical conditions indicating increased risk and suggesting planned birth at an obstetric unit
| Disease Area | Medical Condition |
| Cardiovascular | Confirmed Cardiac Disease Hypertensive disorders |
| Respiratory | Asthma requiring an increase in treatment or hospital treatment Cystic fibrosis |
| Haematological | Haemoglobinopathies such as sickle cell disease,Beta thalassaemia major. History of Thromboembolic disorder. ITP or other platelet disorder . VWD. Bleeding disorder in the woman and unborn baby. Atypical Antibody that carry a risk for haemolytic disease of new born . |
| Endocrine | Hyperthyroidism. Diabetes needing medication. |
| Infective | Hepatitis B or C with abnormal liver function test. Toxoplasmosis – woman receiving treatment .Current active infection of chicken pox ,rubella TB under treatment. |
| Neurological | Epilepsy Myasthenia Gravis. Previous Cerebrovascular Accident . |
| Gastrointestinal | Liver disease associated with current abnormal liver function test. |
| Psychiatric | Psychiatric disorder requiring current in patient care. |
| Immune | SLE. Scleroderma. |
| Renal | Abnormal Renal function test. Renal disease requiring supervision by renal specialist. |
Table 7 Other factors indicating increased risk and suggesting planned birth at an obstetric unit
| FACTORS | Additional Information |
| Previous Complication | Unexplained still birth or neonatal death or previous death related intrapartum difficulty |
| Previous baby with neonatal encephalopathy | |
| Pre eclampsia requiring pre term birth | |
| Placental abruption with adverse outcome | |
| Eclampsia | |
| Primary PPH requiring additional treatment or BT | |
| Caesarean birth | |
| Shoulder Dystocia |
| Factor | Additional Information |
| Current Pregnancy | Placenta praevia |
| Pre-eclampsia or pregnancy-induced hypertension | |
| Preterm labour or preterm prelabour rupture of membranes | |
| Placental abruption | |
| Multiple birth | |
| Anaemia hb less than 85 g/litre at the onset of labor | |
| Confirmed IUFD | |
| Substance misuse | |
| Alcohol dependency requiring assessment or treatment | |
| Gestational diabetes requiring medication | |
| Malpresentation breech or transverse | |
| Recurrent APH | |
| SGA in this pregnancy less than 3rd centile | |
| Abnormal fetal heart rate ,Umbilical or fetal doppler study | |
| Ultrasound diagnosis of Oligo or Polyhydramnios | |
| Previous Gynaecological History | Myomectomy |
| Hysterotomy | |
Compiled By:
Dr. Tahmina Dewan
Contributors
- Prof Fawzia Hossain
- Prof Shahin Ara
- Prof KH Shahnewaz
- Prof Zinat Ara Nasrin
- Dr Taslima Akter
- Dr Sumaiya Binte Asif
- Dr Maniza
- Dr Fariya Shetu
- Dr Umme Rumman
- Dr Amrita Saha
- Dr Lata Dutta
- Dr Tania Akter
- Dr Rubina Akter
- Dr Israt Jahan
