

Key recommendation
Preparation for assisted vaginal birth / Instrumental vaginal delivery/Operative vaginal delivery
Continuous support during labour can reduce the need for assisted vaginal birth.
Epidural analgesia may increase the need for assisted vaginal birth although this is less likely with newer analgesic techniques. [New 2020]
Epidural analgesia in the latent phase of labour compared to the active phase of labour does not increase the risk of assisted vaginal birth. [New 2020]
Women not using epidural adopting upright or lateral positions in the second stage of labour as this reduces the need for assisted vaginal birth.
Women using epidural analgesia adopting lying down lateral positions rather than upright positions in the second stage of labour increases the rate of spontaneous vaginal birth. [New 2020
Delayed pushing for 1-2 hours in nulliparous women with epidural analgesia reduce the need for rotational and midpelvic assisted vaginal birth.
Do not routinely discontinue epidural analgesia during pushing as this increases the woman’s pain with no evidence of a reduction in the incidence of assisted vaginal birth. [New 2020]
There is insufficient evidence to recommend any particular regional analgesia technique in terms of reducing the incidence of assisted vaginal birth. [New 2020]
There is insufficient evidence to recommend routine oxytocin augmentation for women with epidural analgesia as a strategy to reduce the incidence of IVD/OVD.[New 2020]
There is insufficient evidence to recommend routine prophylactic manual rotation of fetal malposition in the second stage of labour to reduce the risk of assisted vaginal birth. [New 2020)
Use a standard classification system for assisted vaginal birth to promote safe clinical practice, effective communication between health professionals and audit of outcomes.
Operators should be aware that no indication is absolute and that clinical judgment is required in all situations.
Suspected fetal bleeding disorders or a predisposition to fracture are relative contraindications to assisted vaginal birth. [New 2020]
Blood borne viral infections in the woman are not an absolute contraindication to assisted vaginal birth. [New 2020]
The use of a vacuum is not contraindicated following a fetal blood sampling procedure or application of a fetal scalp electrode. [New 2020]
Operators should be aware that there is a higher risk of subgaleal haemorrhage and scalp trauma with vacuum extraction compared with forceps at preterm gestational ages. Vacuum birth should be avoided below 32 weeks of gestation and should be used with caution between 32*° and 36*° weeks of gestation. [New 2020
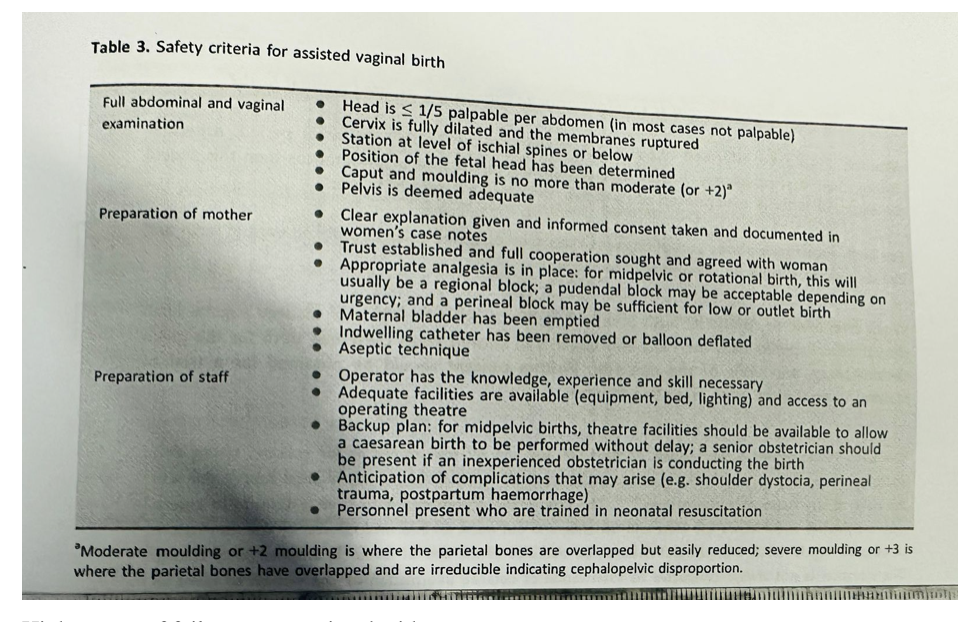
Safe assisted vaginal birth requires a careful assessment of the clinical situation, clear communication with the woman and healthcare personnel, and expertise in the chosen procedure (Table 3).
Ultrasound assessment of the fetal head position prior to assisted vaginal birth is recommended where uncertainty exists following clinical examination. (New 2020)
There is insufficient evidence to recommend the routine use of abdominal or perineal ultrasound for assessment of the station, flexion and descent of the fetal head in the second stage of labour. [New 2020)
Women should be informed about assisted vaginal birth in the antenatal period, especially during their first pregnancy. If they indicate specific restrictions or preferences then this should be explored with an experienced obstetrician, ideally in advance of labour.
For birth room procedures verbal consent should be obtained prior to assisted vaginal birth and the discussion should be documented in the notes.
When midpelvic or rotational birth is indicated, the risks and benefits of assisted vaginal birth should be compared with the risks and benefits of second stage caesarean birth for the given circumstances and skills of the operator. Written consent should be obtained for a trial of assisted vaginal birth in an operating theatre. [New 2020)
Performing assisted vaginal birth
Assisted vaginal birth should be performed by, or in the presence of, an operator who has the knowledge, skills and experience necessary to assess the woman, complete the procedure and manage any complications that arise.
Advise obstetric trainees to achieve expertise in spontaneous vaginal birth prior to commencing training in assisted vaginal birth.
Ensure obstetric trainees receive appropriate training in vacuum and forceps birth, including theoretical knowledge, simulation training and clinical training under direct supervision. [New 2020]
Competency should be demonstrated before conducting unsupervised births. [New 2020]
Complex assisted vaginal births should only be performed by experienced operators or under the direct supervision of an experienced operator.
An experienced operator, competent at midpelvic births, should be present from the outset to supervise all attempts at rotational or midpelvic assisted vagina.
Non-rotational low-pelvic and if out assisted vaginal births have a low probability of failure and most procedures can be conducted safely in a birth room. [New 2020)
Assisted vaginal births that have a higher risk of fallure should be considered a trial and be attempted in a place where immediate recourse to caesarean birth can be undertaken.
The operator should choose the instrument most appropriate to the clinical circumstances and
their level of skill.
Operators should be aware that forceps and vacuum extraction are associated with different benefits and risks; failure to complete the birth with a single instrument is more likely with vacuum extraction, but maternal perineal trauma is more likely with forceps. [New 2020]
Operators should be aware that soft cup vacuum extractors have a higher rate of failure but a lower incidence of neonatal scalp trauma. [New 2020)
Rotational births should be performed by experienced operators; the choice of instrument depending on the clinical circumstances and expertise of the individual. The options include Kielland’s rotational forceps, manual rotation followed by direct traction forceps or vacuum, and rotational vacuum extraction.
Discontinue vacuum-assisted birth where there is no evidence of progressive descent with moderate traction during each pull of a correctly applied instrument by an experienced operator. [New 2020)
Complete vacuum-assisted birth in the majority of cases with a maximum of three pulls to bring the fetal head on to the perineum. Three additional gentle pulls can be used to ease the head out of the perineum. [New 2020)
If there is minimal descent with the first two pulls of a vacuum, the operator should consider whether the application is suboptimal, the fetal position has been incorrectly diagnosed or there is cephalo pelvic disproportion .Less experienced operator should stop and seek a 2nd opinion .Experienced operators should re-evaluate the clinical findings and either change approach or discontinue the procedure. [New 2020]
Discontinue vacuum-assisted birth if there have been two ‘pop-offs’ of the instrument. Less experienced operators should seek senior support after one ‘pop-off’ to ensure the woman has the best chance of a successful assisted vaginal birth. [New 2020]
The rapid negative pressure application for vacuum-assisted birth is recommended as it reduces the duration of the procedure with no difference in maternal and neonatal outcomes. [New 2020]
The use of sequential instruments is associated with an increased risk of trauma to the infant.
However, the operator needs to balance the risks of a caesarean birth following failed vacuum extraction with the risks of forceps birth following failed vacuum extraction.
Obstetricians should be aware of the increased neonatal morbidity following failed vacuum-assisted birth and/or sequential use of instruments, and should inform the neonatologist when this occurs to ensure appropriate care of the baby.
Obstetricians should be aware of the increased risk of obstetric anal sphincter injury (OASI) following sequential use of instruments. [New 2020]
Discontinue attempted forceps birth where the forceps cannot be applied easily, the handles do not approximate easily or if there is a lack of progressive descent with moderate traction. [New 2020]
Discontinue rotational forceps birth if rotation is not easily achieved with gentle pressure. [New 2020]
Discontinue attempted forceps birth if birth is not imminent following three pulls of a correctly applied instrument by an experienced operator. [New 2020]
If there is minimal descent with the first one or two pulls of the forceps, the operator should consider whether the application is suboptimal, the position has been incorrectly diagnosed or there is cephalopelvic disproportion. Less experienced operators should stop and seek a second opinion. Experienced operators should re-evaluate the clinical findings and either change approach or discontinue the procedure. [New 2020)
Obstetricians should be aware of the potential neonatal morbidity following a failed attempt at forceps birth and should inform the neonatologist when this occurs to ensure appropriate management of the baby. [New 2020]
Obstetricians should be aware of the increased risk of fetal head impaction at caesarean birth following a failed attempt at birth via forceps and should be prepared to disimpact the fetal head using recognised manoeuvres. [New 2020]
Mediolateral episiotomy should be discussed with the woman as part of the preparation for assisted vaginal birth. [New 2020]
in the absence of robust evidence to support either routine or restrictive use of episiotomy at assisted vaginal birth, the decision should be tallored to the circumstances at the time and the preferences of the woman. The evidence to support use of mediolateral episiotomy at assisted vaginal birth in terms of preventing OASI is stronger for nulliparous women and for birth via forceps. [New 2020]
When performing a mediolateral episiotomy the cut should be at a 60 degree angle initiated when the head is distending the perineum. [New 2020)
Aftercare following assisted vaginal birth
A single prophylactic dose of intravenous amoxicillin and clavulanic acid should be recommended following assisted vaginal birth as it significantly reduces confirmed or suspected maternal infection compared to placebo. [New 2020]
Good standards of hygiene and aseptic techniques are recommended.
Reassess women after assisted vaginal birth for venous thromboembolism risk and the need for thromboprophylaxis.
In the absence of contraindications, women should be offered regular nonsteroidal anti-inflammatory drugs (NSAIDs) and paracetamol routinely .
Women should be educated about the risk of urinary retention so that they are aware of the importance of bladder emptying in the postpartum period. [New 2020]
The timing and volume of the first void urine should be monitored and documented.
[New 2020]
A post void residual should be measured if urinary retention is suspected.
Recommend that women who have received regional analgesia for a trial of assisted vaginal birth in theatre have an indwelling catheter in situ after the birth to prevent covert urinary retention. This should be removed according to the local protocol. [New 2020]
Offer women physiotherapy-directed strategies to reduce the risk of urinary incontinence at 3 months.
Shared decision making, good communication, and positive continuous support during labour and birth have the potential to reduce psychological morbidity following birth. [New 2020]
Review women before hospital discharge to discuss the indication for assisted vaginal birth, management of any complications and advice for future births. Best practice is where the woman is reviewed by the obstetrician who performed the procedure.
Offer advice and support to women who have had a traumatic birth and wish to talk about their experience. The effect on the birth partner should also be considered. [New 2020]
Do not offer single session, high-intensity psychological interventions with an explicit focus on
reliving the trauma. [New 2020]
Offer women with persistent post-traumatic stress disorder (PTSD) symptoms at 1 month referral to skilled professionals as per the NICE guidance on PTSD. [New 2020]
Inform women that there is a high probability of a spontaneous vaginal birth in subsequent labours following assisted vaginal birth. [New 2020]
Individualise care for women who have sustained a third or fourth-degree perineal tear, or who have ongoing pelvic floor morbidity.
Governance issues
Documentation for assisted vaginal birth should include detailed information on the assessment, decision making and conduct of the procedure, a plan for postnatal care and sufficient information for counselling in relation to subsequent pregnancies. Use of a standardised proforma is recommended. [New 2020]
Paired cord blood samples should be processed and recorded following all attempts at assisted vaginal birth. [New 2020]
Adverse outcomes, including unsuccessful assisted vaginal birth, major obstetric haemorrhage, OASI, shoulder dystocia and significant neonatal complications should trigger an incident report as part of effective risk management processes. [New 2020]
Obstetricians should ensure that the ongoing care of the woman, baby and family is paramount. [New 2020]
Obstetricians have a duty of candour; a professional responsibility to be honest with patients when things go wrong. [New 2020)
Obstetricians should contribute to adverse event reporting, confidential enquiries, and take part in regular reviews and audits. They should respond constructively to outcomes of reviews, taking necessary steps to address any problems and carry out further retraining where needed.
[New 2020]
Maternity units should provide a safe and supportive framework to support women, their families and staff when serious adverse events occur. [New 2020]
Assisted vaginal birth by vacuum or forceps is used to assist birth for maternal and fetal indications. In the UK, between 10% and 15% of all women give birth by assisted vaginal birth.’ Almost one in every three nulliparous women gives birth by vacuum or forceps, with lower rates in midwifery-led care settings23 There has been a rise in the rate of caesarean births in the second stage of labour; this may reflect concerns about assisted vaginal birth morbidity or a loss of clinical skills.*
TABLE 1
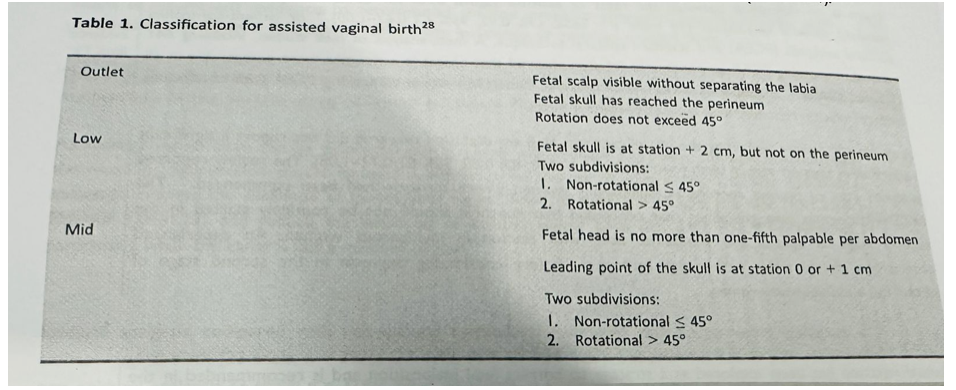
TABLE 2
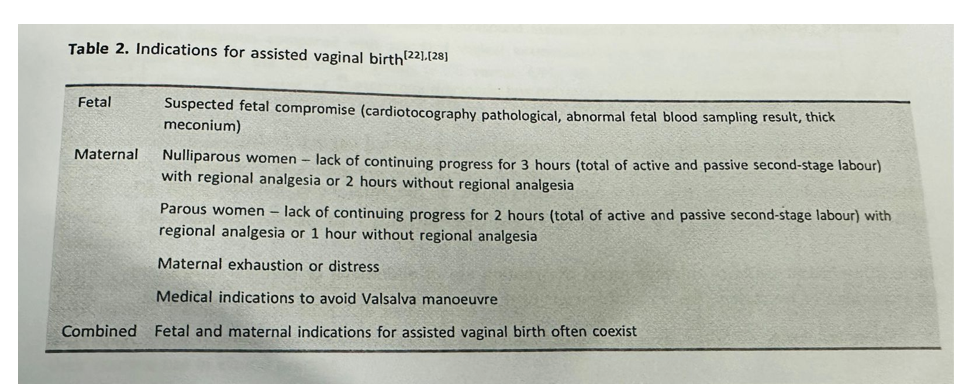
TABLE 3
Higher rates of failure are associated with:
* maternal BMI greater than 30
* short maternal stature
* estimated fetal weight of greater than 4 kg or a clinically big baby
* head circumference above the 95th percentile
* occipito-posterior position
* midpelvic birth or when one-fifth of the head is palpable per abdomen.
TABLE 4
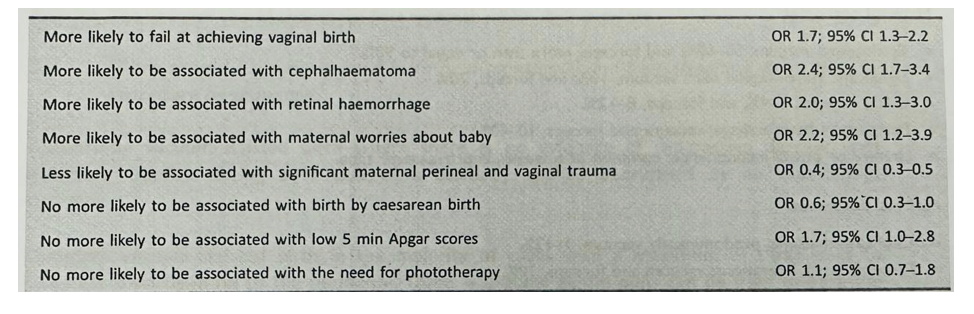
Risk-based information can be summarised as follows:”
Maternal outcomes:
* Episiotomy, vacuum, 50-60%; and forceps, more than or equal to 90%.
* Significant vulvo-vaginal tear; vacuum, 10%; and forceps, 20%.
* OASI; vacuum, 1-4%; and forceps, 8-12%.
* Postpartum haemorrhage; vacuum and forceps, 10-40%.
* Urinary or bowel incontinence; common at 6 weeks, improves over time.
Perinatal outcomes:
* Cephalhaematoma; predominantly vacuum, 1-12%.
* Facial or scalp lacerations; vacuum and forceps, 10%.
Retinal haemorrhage; more common with vacuum than forceps, variable 17-38%.
Jaundice or hyperbilirubinaemia; vacuum and forceps, 5-15%.
* Subgaleal haemorrhage; predominantly vacuum, 3 to 6 in 1000.
* Intracranial haemorrhage; vacuum and forceps, 5 to 15 in 10 000.
* Cervical spine injury; mainly Kiellands rotational forceps, rare.
* Skull fracture; mainly forceps, rare.
* Facial nerve palsy; mainly forceps, rare.
* Fetal death; very rare.
Compiled By:
Dr. Tahmina Dewan
Contributors
- Prof Fawzia Hossain
- Prof Shahin Ara
- Prof KH Shahnewaz
- Prof Zinat Ara Nasrin
- Dr Taslima Akter
- Dr Sumaiya Binte Asif
- Dr Maniza
- Dr Fariya Shetu
- Dr Umme Rumman
- Dr Amrita Saha
- Dr Lata Dutta
- Dr Tania Akter
- Dr Rubina Akter
- Dr Israt Jahan
