

Introduction
Purpose: To provide standardized, evidence-based guidance for diagnosis and management of Gestational Trophoblastic Disease across Bangladesh
Scope: Applicable to all healthcare facilities
Alignment: Adapted from international guidelines (Practical Guidelines for the Treatment of Gestational Trophoblastic Disease: Collaboration of the European Organization for the Treatment of Trophoblastic Disease (EOTTD)–European Society of Gynaecologic Oncology (ESGO)–Gynecologic Cancer Intergroup (GCIG) International Society for the Study of Trophoblastic disease (ISSTD), FIGO) and contextualized to local resources, culture and health system Capacity.
Definition
Gestational trophoblastic diseases (GTDs) are a group of rare premalignant and malignant diseases characterized by their origin in trophoblastic cells.
Premalignant forms are complete (CHM), partial hydatidiform moles (PHM), and atypical placental site nodules (APSNs). Malignant forms are called gestational trophoblastic neoplasia (GTN) and include invasive mole, choriocarcinoma, placental site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor (ETT).
Diagnostic and Management Pathways
Hydatidiform mole (HM) can be suspected when severe hyperemesis or symptoms of hyperthyroidism occur, patients present with vaginal bleeding or are asymptomatic and undergo first trimester ultrasound (US).
Minimal requirements
- Ultra sound
- Suspect HM or HM not excluded
- Serum hCG
- Blood group and save for crossmatch, CXR, S.TSH
- Suction curettage under anesthesia
- Ultra Sound or hysteroscopy to ensure complete evacuation
- Consider oxytocin
- Cervical ripening can be considered
- In selected cases, hysterectomy is an option
- Send tissue for histology
Follow up:
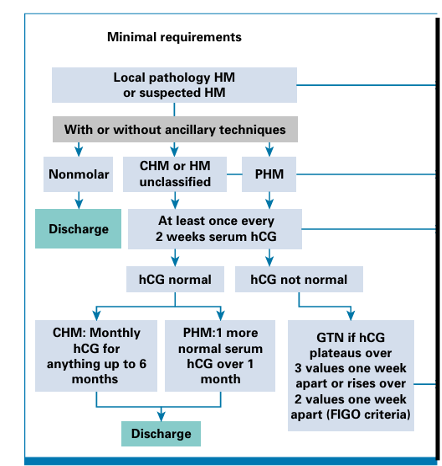
Fig: Follow up and diagnostic pathway for HM to GTN
FIGO criteria for diagnosis of Post molar gestational trophoblastic neoplasia
When the plateau of hCG lasts for four measurements over a period of 3 weeks or longer; that is, days 1, 7, 14, 21.
• When there is a rise in hCG for three consecutive weekly measurements over at least a period of 2 weeks or more; days 1, 7, 14.
• If there is a histologic diagnosis of choriocarcinoma
FIGO staging and classification for gestational trophoblastic neoplasia
I: Gestational trophoblastic tumors strictly confined to the uterine corpus
II: Gestational trophoblastic tumors extending to the adnexae or to the vagina, but limited to the genital structures
III: Gestational trophoblastic tumors extending to the lungs, with or without genital tract involvement
IV: All other metastatic sites
0 1 2 4
Age <40 >40
Scoring system based on prognostic factors
| Prognostic Factor | 0 | 1 | 2 | 4 |
|---|---|---|---|---|
| Antecedent pregnancy | mole | abortion | term | |
| Interval month from index pregnancy | <4 | 4-<7 | 7->13 | >13 |
| Pretreatment serum hCG | <1000 | 1000-<10,000 | 10,000-1,00,000 | >100,000 |
| Largest tumor size | 3-<5 cm | >5 cm | ||
| Site of metastasis | lung | Kidney/spleen | Gastrointestinal/ | Liver/brain |
| No of metastasis | – | 1-4 | 5-8 | >8 |
| Previous failed chemotherapy | – | – | Single drug | 2 or > drugs |
Staging of postmole GTN
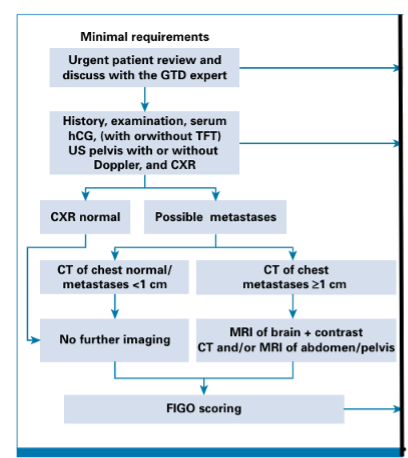
Fig: Post mole GTN staging
Treatment of Postmole GTN
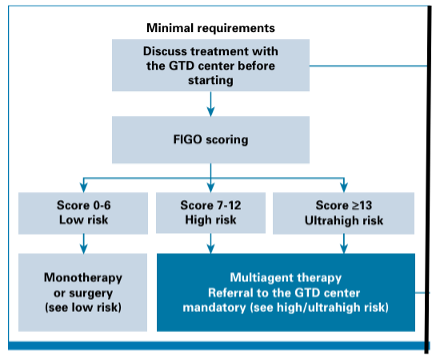
Fig: Postmole GTN treatment
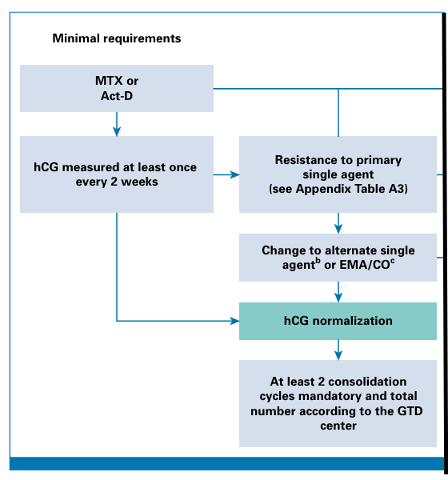
Treatment of Low risk GTN to remission
High risk GTN Treatment to Remission
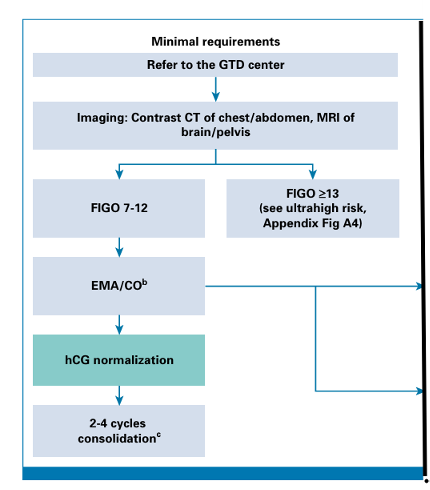
Treatment of Ultra High risk GTN

Follow up of Low Risk GTN
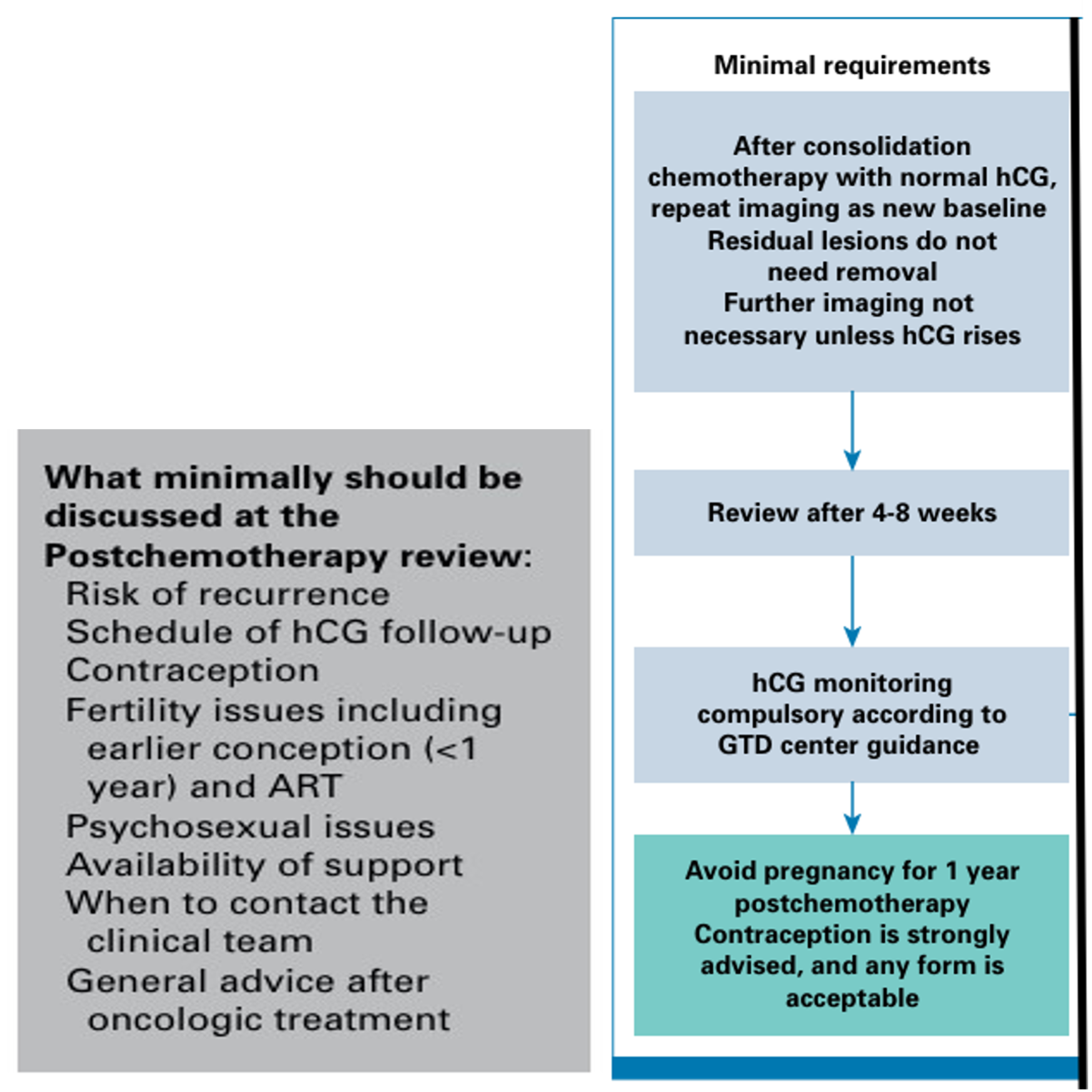
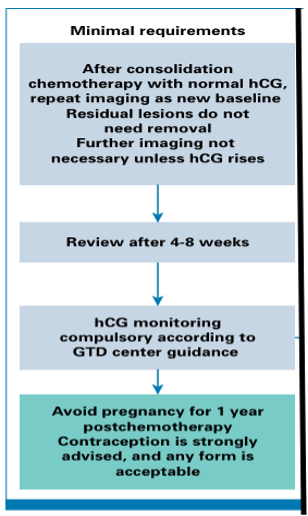
Followup of High risk GTN and Ultra High risk GTN
Compiled By
Dr. Farhana Kalam
MBBS (DMC), FCPS (OBGYN)
FCPS (Gynae Oncology)
Contributors
1. Prof Fawzia Hossain
2. Prof KH Shahnewaz
3. Dr Maniza Khan
4. Dr Sumaiya Binte Asif
5. Dr Ananna Zakia
6. Dr Lutfa Amin
7. Dr Tasrina Akhter
8. Dr Amrita Saha
9. Dr Farjana Sultana
10. Dr Afroza Akhter
