

Introduction
Cervical cancer is the 4th most common cancer in women worldwide and the 2nd in incidence and mortality in developing countries.
Over 300,000 women died from cervical cancer globally in 2018; more than 90% of deaths were in low- and middle-income countries.
It is caused primarily by persistent infection with high-risk HPV. It is largely preventable through vaccination, lifestyle modification, and screening. Screening significantly reduces incidence and mortality.
HPV is responsible for 99.7% of cervical cancer cases, and although over 80% of women will become infected with HPV at some point during their lives, the majority of infections are cleared (become DNA negative) on their own. Thus, HPV is necessary but not sufficient for cervical cancer development; persistent infection with HPV can lead to cervical precancer over the course of around 5–10 years, and in around 20 years can develop into cancer. The long interval between HPV infection and cancer development, as well as the anatomical position of the cervix being suitable for non-invasive sampling, mean that cervical cancer screening is beneficial and cost-effective at a population level.
Risk Factors and Cofactors
Cofactors are necessary for progression from cervical HPV infection to cancer which includes:
- Early onset of sexual activity
- Long-term use of oral contraceptives
- Multiparity
- Age at first full-term pregnancy
- Tobacco exposure
- Immunosuppression
About HPV
HPV is a small, non-enveloped, double-stranded DNA virus.
Shows a specific tropism for human epithelial cells in the skin and mucous membranes.
100 genotypes identified which infect human epithelium.
Based on the potential to cause malignancy HPV can be grouped to High-Risk (HR) and Low-Risk (LR) type.
Low risk or non-oncogenic HPV types are not associated with cancer, but can cause Low grade cervical abnormalities or benign proliferative warts (HPV 6 and 11)
Approximately 14-18 are HR-HPV or oncogenic HPV
HPV 16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82 are associated with anogenital dysplasias having a potential for progression to cancer.
They are responsible for about-
60–90% of vaginal and anal cancers
50% of vulvar cancers
25- 60% of head and neck cancers
99.7% cervical cancer.
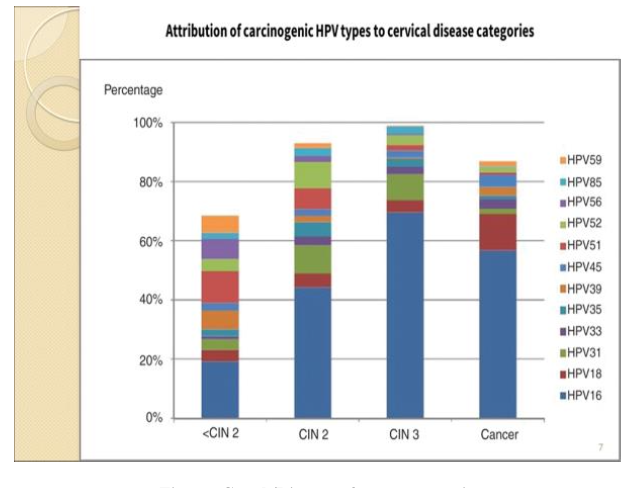
Globally, about 70% of cervical cancers are associated with two HR-HPV types 16/18.
In Bangladesh, HPV16 detected in 82% and type 18 in 9% cases of cervical cancers.
Figure: Graph/Diagram from presentation
Pathophysiology
- HPV infection of cervical epithelium
- Development of cervical intraepithelial neoplasia (CIN)
- Progression from CIN I → CIN III → invasive carcinoma if untreated
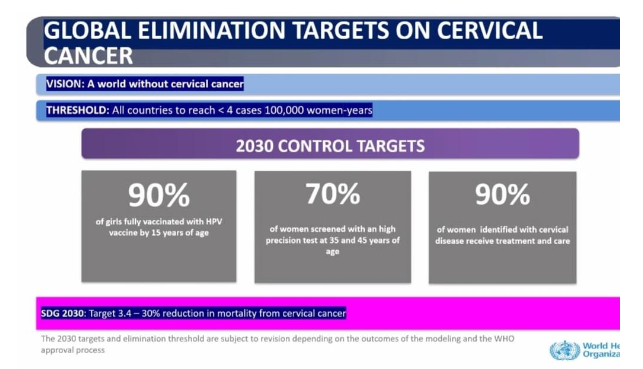
WHO Elimination Strategy (90–70–90)
Cervical Cancer Prevention
Primary Prevention
Focuses on preventing HPV infection and reducing risk factors.
a) HPV Vaccination:
Most effective preventive strategy.
Available vaccines: Bivalent, Quadrivalent, and Nonavalent (covering HPV types 16, 18, and more).
WHO recommends vaccination for girls aged 9–14 years, before sexual debut.
Boys can also be vaccinated to reduce transmission
b) Health Education and Awareness:
Promoting knowledge about HPV, safe sexual practices, and cervical cancer.
Public health campaigns to increase vaccine uptake.
c) Lifestyle Modifications:
- Delaying onset of sexual activity.
- Limiting multiple sexual partners.
- Condom use (reduces HPV transmission, though not fully protective).
- Avoidance of smoking (linked to higher risk of cervical neoplasia).
Secondary Prevention
Screening and treatment of preinvasive disease of cervix.
Screening: Early detection of precancerous lesions before progression to invasive cancer.
Three approaches for cervical cancer screening:
| Screening Test | Molecular | Cytologic | Visual Inspection |
|---|---|---|---|
| Test | High risk HPV DNA test, DNA methylation test, Protein biomarkers (HPV antibody test, oncoprotein test E6/E7), Dual staining p16/Ki67 | Conventional Pap smear, Liquid based cytology | VIA, VILI |
Why High-risk HPV DNA test taken as primary screening test:
- Very high sensitivity: 90-100%
- Specificity: 90-95%
- Negative predictive value near 100%
Screening Guidelines
WHO 2021 Guideline:
- Start screening at age 30 years. 25 years for HIV positive patient.
- Primary screening test: HPV DNA test
- Triage test: Cytology/colposcopy/partial genotyping
- Screening interval: every 5–10 years if HPV test is negative. 3–5 years for HIV positive patient.
- Continue up to age 50–65, depending on national protocols.
RCOG (Green-top) Guidelines – UK (2019):
- Starting Age: 25 years.
- Screening Intervals: 25–49 years: every 3 years; 50–64 years: every 5 years; Age 65+: only if not previously screened or had abnormal results in past 10 years.
- Screening Method: HPV primary testing (since 2019) with reflex cytology.
- HPV negative → return to routine recall
- HPV positive → cytology; abnormal → colposcopy
- HPV positive but cytology normal → repeat in 12 months
- Special Groups: Symptomatic women, immunosuppressed, post-hysterectomy with history of CIN/cancer
USPSTF Guidelines (2018):
- Start at 21 years of age
- 21–29: cytology every 3 years
- 30–65: HPV test every 5 years OR co-testing every 5 years OR cytology alone every 3 years
- Stop at 65 if adequate prior screening and no high-risk factors
- After hysterectomy: no screening if cervix removed and no history of CIN2 or cancer
Australian National Cancer Screening Program (NCSP) for Cervical cancer 2022:
- Primary screening test: HPV DNA test
- Triage tests: Reflex LBC
- Age of screening: 25-74 years
- Screening interval: 5-years
In Bangladesh:
- Primary screening test: VIA
- Secondary screening test: Colposcopy
Newer concept: Self sampling
- Self-sampling (vaginal swabs by patient) may improve coverage and participation, especially for non-attenders.
- Under-screened women are at higher risk of invasive cancer.
- Large meta-analyses found self-sampling similarly accurate to clinician-taken samples.
Tertiary Prevention (Management & Treatment)
Preventing complications and mortality from established disease.
a) Treatment of precancerous lesions: Cryotherapy, LEEP, Conization
b) Management of invasive cancer: Surgery, radiotherapy, chemotherapy depending on stage
c) Palliative care: Improves quality of life in advanced cases
Conclusion
Cervical cancer is highly preventable through HPV vaccination and regular screening. Public health efforts must focus on awareness, accessibility, and affordability, aiming to meet WHO elimination targets by 2030.
References
- World Health Organization. Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem. WHO, 2020.
- International Agency for Research on Cancer. Cancer Today: Cervical Cancer Statistics. IARC, 2020.
- American College of Obstetricians and Gynecologists (ACOG). Cervical Cancer Screening Guidelines, 2021.
- Royal College of Obstetricians and Gynaecologists (RCOG). Cervical Screening (Green-top Guidelines), 2019.
- Bangladesh Cervical Cancer Screening Program – Ministry of Health, 2021.
- Maucort-Boulch D, Franceschi S, Plummer M, IARC HPV Prevalence Surveys Study Group. International correlation between human papillomavirus prevalence and cervical cancer incidence. Cancer Epidemiol Biomarkers Prev. 2008;17(3):717–720.
- IARC. Cervix cancer screening. In: Strategies IWGatEoCP, ed. IARC Handbooks of Cancer Prevention. Volume 10. Lyon: IARC Press; 2005
- Ho GY, Bierman R, Beardsley L, et al. Natural history of cervicovaginal papillomavirus infection in young women. N Engl J Med. 1998;338(7):423–428
- Mitchell MF, Tortolero-Luna G, Wright T, et al. Cervical human papillomavirus infection and intraepithelial neoplasia: A review. J Natl Cancer Inst Monogr. 1996(21):17–25
- Ostor AG. Natural history of cervical intraepithelial neoplasia: A critical review. Int J Gynecol Pathol. 1993;12(2):186–192.
- Wang SS, Zuna RE, Wentzensen N, et al. Human papillomavirus cofactors by disease progression and human papillomavirus types in the study to understand cervical cancer early endpoints and determinants. Cancer Epidemiol Biomarkers Prev. 2009;18:113–120.
- Middleton K, Peh W, Southern S, et al. Organization of human papillomavirus productive cycle during neoplastic progression provides a basis for selection of diagnostic markers. J Virol. 2003;77(19):10186–10201
- Castle PE, Sideri M, Jeronimo J, et al. Risk assessment to guide the prevention of cervical cancer. Am J Obstet Gynecol. 2007;197(4):1–6
- McCredie MR, Sharples KJ, Paul C, et al. Natural history of cervical neoplasia and risk of invasive cancer in women with cervical intraepithelial neoplasia 3: A retrospective cohort study. Lancet Oncol. 2008;9:425–434
Compiled By:
Dr. Nazmun Nahar Nabiha
Dr. Sayema Tabassum
Contributors
- Prof Dr Fawzia Hossain
- Dr Tasnuva Akhter
- Dr Maniza Khan
- Dr Nurun Nahar
- Dr Ananna Zakia
- Dr Lutfa Amin
- Dr Tasrina Akhter
- Dr Amrita Saha
- Dr Lutfa Akhter
- Dr Aklima Zakaria Zinan
