

Introduction
Causes of infertility are equality distributed between the sexes. So, combined factors need to evaluate.
Clinical definition (WHO):
- Infertility: A disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse.
- Subfertility: is used interchangeably to describe women or couples, who may not be sterile but exhibit decreased reproductive efficiency.
Prevalence: (Gender distribution)
Multinational study by WHO:
- Female fertility : 37% of infertility couple.
- Male fertility : 8% of infertility couple.
- Both : 35% of infertile couple.
ARSM 2022:
- Male – 40% of infertility
- Female – 40% of infertility
- Unexplained – 20%
When a couple need to start investigations:
ASRM initiation:
years.
- Failure to achieve pregnancy within 12 months of unprotected inter course in young <35
Or - Within 6 months in older woman >35 years.
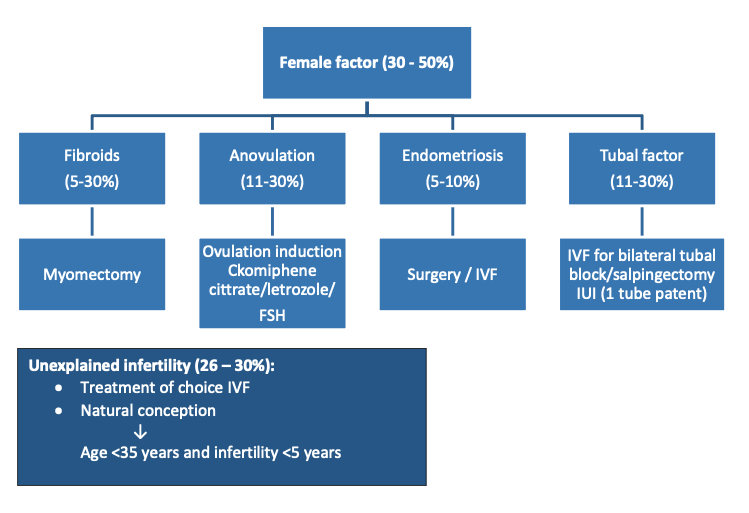
Common identifiable factors: (WHO 2022)
- Ovulatory disorder : 25%
- Endometriosis : 15%
- Pelvic adhesion : 12%
- Tubal block : 11%
- Uterine anomaly : 11%
- Hyperprolactinaemia : 7%
History & physical examination:
- Duration of Infertility
- Obstetrical history
- Menstrual history, including molimina
- Medical, surgical, and gynecological history including a sexually transmitted infection
- Sexual history to include coital frequency and timing
- Focusing on the male partner including ejaculation problem
- Social and lifestyle history to include cigarettes, alcohol, exercise, diet and occupation
- Family history, screening for genetic issues, recurrent pregnancy loss and infertility.
Female and male infertility risk factors:
| Both genders | Female |
|---|---|
| Family history of infertility | Age >35 years |
| Recurrent abortions | Reduced ovarian reserve |
| Obesity | Ovulation Disorders |
| Using of anabolic steroids | Infertility >3 years |
| Lifestyles | Menstrual disorders |
| Environmental/occupational factors | Endometriosis |
Physical examinations:
- Vital signs and body mass index
- Thyroid evaluation
- Breast examinations for galactorrhea
- Signs of androgen excess
- Abnormal vaginal or cervical anatomy
- Pelvic masses or tenderness
- Uterine enlargement or irregularity.
Investigations:
5 initial investigations category: (WHO, ASRM, ESHRE)
A) Ovarian reserve test (ORT)
B) Uterine cavity assessment
C) Tubal assessment
D) Endocrinological blood test
E) Semen
When & how to do:
A) Ovarian reserve test (ORT):
- Day 2:
- FSH
- AMH
- AFC
- Estradiol (E2)
AMH is a hormone expressed by preantral and antral follicles, representing a marker of ovarian function that can be mounted at any time during a woman’s cycle.
AMH levels gradually decline throughout a woman’s natural reproductive life to undetectable levels at menopause. AMH levels seem to be a good predictor of exogenous gonadotropin response:
- 1.0 to 3.5 ng/ml : Normal values
- Less than 0.5 ng/ml : Predicts difficulty getting more than 3 follicle to grow
- Less than 1.0 ngml : Require more aggressive ovulation induction protocols
- Greater than 3.5 ng/mL : Require mild induction to prevent hyperstimulation.
Ovarian reserve testing can be only justified for women with any of the following characteristics:
- Age over 35
- Unexplained ovarian reserve infertility to identify unsuspected loss of ovarian reserve
- Family history of early menopause
- Previous ovarian surgery (ovarian cystectomy or drilling, unilateral oophorectomy)
- Chemotherapy or radiation
- Smoking
- Demonstrated poor response to exogenous gonadotropin stimulation
[ESHRE]
B) Tubal Evaluation:
Indications for tubal patency testing:
- Diagnosis of infertility or having trouble conceiving for 6 to 12 months without success.
- History of multiple miscarriages.
- History of conditions such as endometriosis, ectopic pregnancy or pelvic infections.
- History of sexually transmitted infections (STI) like chlamydia or gonorrhea.
- Post-operative assessment following tubal surgery, such as a tubal ligation or its reversal.
- Before new assisted reproductive treatments.
[ESHRE]
Methods:
- The gold standard for the evaluation of tubal patency is laparoscopy with chromopertubation.
- The hysterosalpingogron (HSG) is more commonly used for the first-line evaluation for tubal petency as less invasive.
- Saline infusion sonography (SIS)
C) Uterine Cavity:
- Transvaginal sonography (TVS) [on day 2 of the menstrual cycle]
- The gold standard for assessing the uterine cavity is hysteroscopy which allows direct visualization of the intrauterine pathology and provides an opportunity for immediate surgical correction.
- Saline infusion sonogram (SIS).
D) Endocrinological & routine blood test:
| Investigations for a female partner | Investigations for a male partner |
| CBC, ESR | Semen analysis |
| Blood sugar levels | Blood sugar levels |
| Hormone profile (on day 2 of the menstrual cycle) FSH, LH, prolactin (irregular mens), TSH | Screening for HIV, VDRL, HCV, HBsAg |
| Screening for HBsAg, VDRL, HIV, HCV | FSH, LH (if indicated) |
| Urine exam (routine and microscopic) |
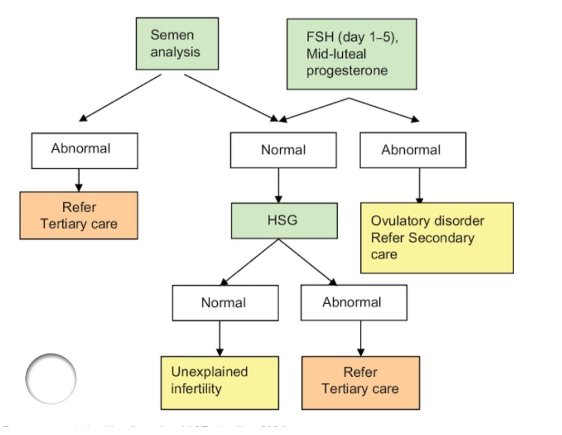
Diagnostic approach to infertility in the woman:
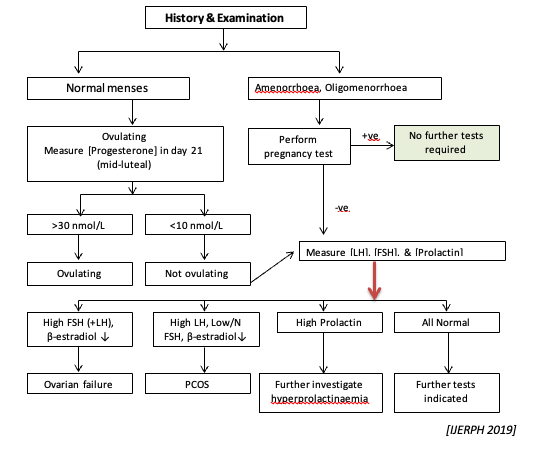
When to start ovulation inducing drug (OID):
- Only with evidence of anovulation
- No specific BMI is required to initiate fertility treatment, (5 – 10) % weight reduction restore ovulation in (50 – 100) % of woman within 1 year.
(ACOG, ASRM, WHO)
1st line medication for ovulation induction:
- Aromatase inhibitor 1st choice for PCOS (ACOG): 2.5 mg to 7.5 mg.
- Clomiphene citrate (for type II anovulation) [SERM]: not for I & III (50 mg to 150 mg)
↓ - Who fail to conceive after multiple cycle of clomiphene or letrozole
↓
Gonadotropin – for type 1, 2, 3 anovulation
(Serial TVS)
↓
Follicle >18 mm with E2 >200 pg/ml
↓
Trigger
36 hours after trigger
↓
IUI (failed 3 – 4 cycle)
↓
IVF
Management of the infertile female:
Male infertility workup:
Semen: Who laboratory manual 2022
| Parameter | 5ᵗʰ centile data |
|---|---|
| Semen volume | > 1.4 ml |
| Semen conc x 10⁶/ml | ≥ 16 million |
| Total sperm no. x 10⁶ /ejac | ≥ 39 million |
| TM (PR+NP) % | ≥ 42 % |
| PR% | ≥ 30 % |
| NP% | 1 % |
| IM% | 20 % |
| Vitality % | ≥ 54 % |
| Normal forms % | ≥ 4.0% |
| Leucocytes | 1 – 2 x 10⁶/ml |
Male Factor Algorithm:
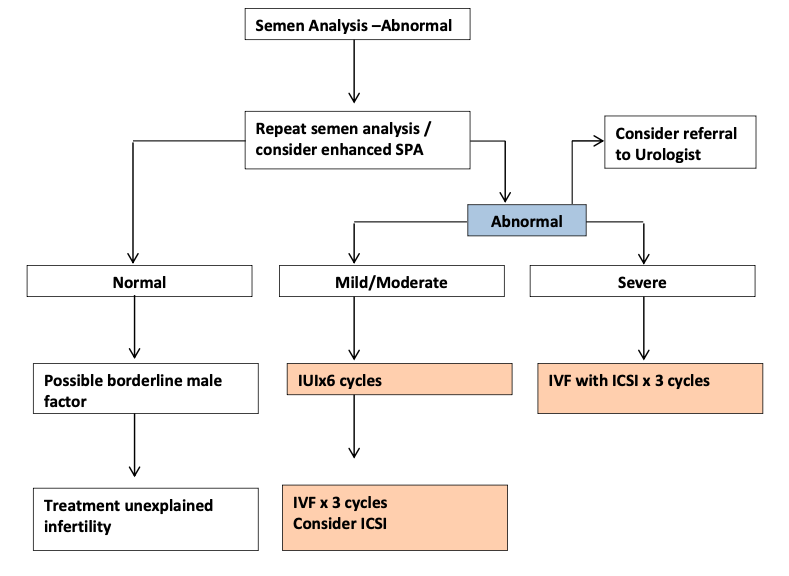
When to refer:
Refer to ART centre:
- Severe male factor
- Uterine cavity distortion
- DOR
- Tubal occlusion
- Recurrent IUI failure
- Unexplained infertility
Implementation:
- Timely referral to ART centre
- Refresher training
- Adherence with guideline
- Patient education
- Enhancing health care team outcome
Data alignment:
Identified by database search:
- PUBMED
- MEDLINE
- GOOGLE SCHOLAR
- ARTICLE.
References:
- Chandra A, Copen CE, Stephen EH. Infertility and impaired fecundity in the United States, 1982-2010: data from the National Survey of Family Growth. Natl Health Stat Report. 2013 Aug 14;(67):1-18, 1 p following 19. [PubMed]
- Richardson SJ, Senikas V, Nelson JF. Follicular depletion during the menopausal transition: evidence for accelerated loss and ultimate exhaustion. J Clin Endocrinol Metab. 1987 Dec;65(6):1231-7. [PubMed]
- Pritts EA. Fibroids and infertility: a systematic review of the evidence. Obstet Gynecol Surv. 2001 Aug;56(8):483-91. [PubMed]
- GUTTMACHER AF. Factors affecting normal expectancy of conception. J Am Med Assoc. 1956 Jun 30;161(9):855-60. [PubMed]
- Practice Committee of the American Society for Reproductive Medicine. Definitions of infertility and recurrent pregnancy loss: a committee opinion. Fertil Steril. 2013 Jan;99(1):63. [PubMed]
- Practice Committee of American Society for Reproductive Medicine in collaboration with Society for Reproductive Endocrinology and Infertility. Optimizing natural fertility. Fertil Steril. 2008 Nov;90(5 Suppl):S1-6. [PubMed]
- Wathen NC, Perry L, Lilford RJ, Chard T. Interpretation of single progesterone measurement in diagnosis of anovulation and defective luteal phase: observations on analysis of the normal range. Br Med J (Clin Res Ed). 1984 Jan 07;288(6410):7-9. [PMC free article] [PubMed]
- Ecochard R, Boehringer H, Rabilloud M, Marret H. Chronological aspects of ultrasonic, hormonal, and other indirect indices of ovulation. BJOG. 2001 Aug;108(8):822-9. [PubMed]
- Seshadri S, El-Toukhy T, Douiri A, Jayaprakasan K, Khalaf Y. Diagnostic accuracy of saline infusion sonography in the evaluation of uterine cavity abnormalities prior to assisted reproductive techniques: a systematic review and meta-analyses. Hum Reprod Update. 2015 Mar-Apr;21(2):262-74. [PubMed]
- Abraham S, Mira M, Llewellyn-Jones D. Should ovulation be induced in women recovering from an eating disorder or who are compulsive exercisers? Fertil Steril. 1990 Mar;53(3):566-8. [PubMed]
- ACOG Committee Opinion No. 738: Aromatase Inhibitors in Gynecologic Practice. Obstet Gynecol. 2018 Jun;131(6):1. [PubMed]
- Casper RF, Mitwally MF. Review: aromatase inhibitors for ovulation induction. J Clin Endocrinol Metab. 2006 Mar;91(3):760-71. [PubMed]
- Reindollar RH, Regan MM, Neumann PJ, Levine BS, Thornton KL, Alper MM, Goldman MB. A randomized clinical trial to evaluate optimal treatment for unexplained infertility: the fast track and standard treatment (FASTT) trial. Fertil Steril. 2010 Aug; 94(3):888-99. [PubMed]
- Practice Committee of the American Society for Reproductive Medicine. Use of clomiphene citrate in infertile women: a committee opinion. Fertil Steril. 2013 Aug; 100(2):341-8. [PubMed]
- Golan A, Ron-el R, Herman A, Soffer Y, Weinraub Z, Caspi E. Ovarian hyperstimulation syndrome: an update review. Obstet Gynecol Surv. 1989 Jun;44(6):430-40. [PubMed].
Compiled By
Dr. Rubina Akter
Contributors
1. Prof Fawzia Hossain
2. Prof KH Shahnewaz
3. Dr Maniza Khan
4. Dr Sumaiya Binte Asif
5. Dr Ananna Zakia
6. Dr Lutfa Amin
7. Dr Tasrina Akhter
8. Dr Amrita Saha
9. Dr Farjana Sultana
10. Dr Afroza Akhter
