

Identification and Management of Maternal Sepsis During and Following Pregnancy
| Full title | Identification and Management of Maternal Sepsis During and Following Pregnancy |
| Author | Tasrina Akter |
| Scope (Target audience) | Clinicians, Obstetrician, midwives, microbiologist |
| Review date | October 2025 |
| Patient group to which it applies | This guideline should be applied to all pregnant women and postnatal (up to 6 weeks) women |
| NICE guideline reference | N/A |
| Summary of evidence base this guideline has created from | RCOG green top guideline 64 |
| Contents | |
| 1. Introduction | 2 |
| 2. AIMS | 2 |
| 3. Objectives | 2 |
| 4. Definitions | 2 |
| 5. Risk factors and potential causes of maternal sepsis | 3 |
| 6. Prevention of sepsis | 4-5 |
| 7. Recognition of maternal sepsis | 5-11 |
| 8. Management of red flag sepsis | 11-16 |
| 9. Deteriorating women with sepsis | 17-18 |
| Appendix 1 | 18 |
| Appendix 2 | 19 |
| Appendix 3 | 20 |
| Appendix 4 | 21 |
| Appendix 5 | 22 |
1. Introduction
Sepsis during and following pregnancy remains an important cause of maternal death globally, accounting for 11% of all maternal deaths.
The overall incidence rate of puerperal (postpartum) sepsis in Bangladesh is 4.5 per 100 live births, according to available data. However, this rate can vary significantly, with hospital-based studies showing higher rates of maternal mortality due to puerperal sepsis, such as 17 and 20.3 per 100 live births in two different government hospitals.
Any obstetric woman with suspected sepsis will require urgent clinical review, multi- disciplinary care, prompt treatment and action. Failure to recognize sepsis early is a significant cause of preventable morbidity, resulting in delayed treatment and escalated care, which are critical if lives are to be saved.
2. AIMS
This guideline had been developed to provide all healthcare professionals caring for pregnant and postpartum women (up to 6 weeks postnatal) with evidence-based
information relating to the early recognition, diagnosis and management of sepsis in order to prevent further deterioration and improve outcomes. As healthcare
professionals we should aim to:
- Prevent sepsis with the appropriate use of prophylactic antibiotics
- Recognize sepsis and treat promptly following the Sepsis Six pathway.
3. OBJECTIVES
To ensure that all healthcare professionals providing care to pregnant and postnatal women:
- Receive guidance on prevention, recognition treatment and escalation of women presenting with signs of sepsis.
- Have the knowledge base to provide education to our parents about the signs and symptoms of sepsis, especially in the home environment.
4. DEFINITIONS
In 2017 the World Health Organization defined maternal sepsis as “a life-threatening condition defined as organ dysfunction resulting from infection during pregnancy, childbirth, post-abortion, or postpartum period.” This definition is aligned with the current international consensus definition of adult sepsis and supersedes the prior use of the term sepsis to describe infection that has caused a systemic inflammatory response (SIRS).
Septic shock is now described as a clinical construct of sepsis with persisting hypotension requiring vasopressors to maintain an adequate blood pressure (MAP 65 mm Hg or more), alongside a persistent serum lactate (either venous or arterial) level more than2 mmol/L despite adequate volume resuscitation.
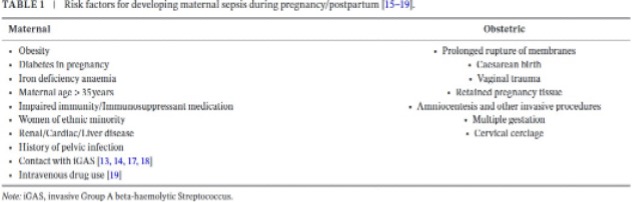
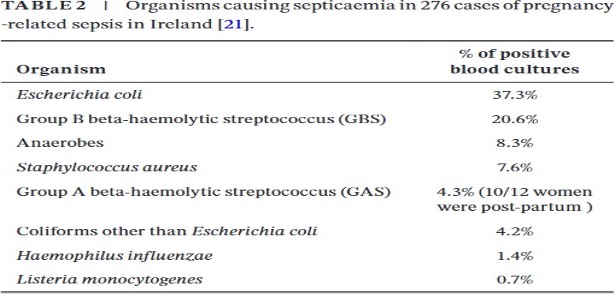
5. RISK FACTORS & POTENTIAL CAUSES OF MATERNAL SEPSIS
Many women who present with sepsis will have no risk factors. Table 1 below reveals pregnancy related and non-pregnant risk factors whilst table 2 showing common organisms causing sepsis in pregnancy.
6. PREVENTION OF SEPSIS
6.1. Antenatal
- Influenza vaccination: MBRRACE-UK, (2014), revealed that 1 in 11 maternal deaths were due to influenza infections. All women who are pregnant during the influenza season, regardless of stage of pregnancy, should be offered the inactivated influenza vaccine. To avoid preventable deaths, the benefits of influenza vaccination to pregnant women should be promoted and pregnant women at any stage of pregnancy should be offered vaccination.
- Advice to at risk women: All women should be informed of the risks, signs and symptoms of infection and the need for them to seek early advice if they are concerned. Offer appropriate and clear advice on infection prevention and symptom identification in situations where women are at risk of sepsis e.g. premature rupture of membranes.
The first signs of sepsis are usually a rise in temperature, heart rate and breathing. The woman may also feel unwell; have chills and flu-like symptoms abdominal pain and / or diarrhoea. Also see section 6.3.1 below.
- Prophylactic antibiotics: Prophylactic antibiotics should be prescribed and administered for women at risk of sepsis e.g. PPROM, caesarean section, recurrent urinary tract infections
- Group A streptococcus: Many of the deaths from genital tract sepsis in the Confidential Enquires were caused by group A Streptococcus (GAS). The bacterium is commonly carried on the skin and nasal passages. It can cause localized upper respiratory tract infections (tonsillitis, pharyngitis) or skin infections (impetigo). Pregnant and postpartum women however can be vulnerable to invasive infection which can rapidly lead to an overwhelming sepsis.
Any GAS identified during pregnancy should be treated to avoid invasive GAS infection. The presence of three or four of the following signs suggests that a woman may have a bacterial infection and would benefit from antibiotics: tonsillar exudate, tender anterior cervical lymphadenopathy or lymphadenitis, fever and absence of cough.
6.2 Intrapartum
- Prophylactic antibiotics for Group B Streptococcus: Women with a GBS positive swab should have intrapartum antibiotics prophylaxis.
- Group A streptococcus (GAS): Empiric treatment should cover Group A streptococcus. If Group A Streptococcus is isolated this should be discussed with the Microbiologist who will advise on the choice of appropriate antibiotic therapy. This will decrease the risk of invasive GAS infection. Neonatologists should be informed of any
GAS finding in mother as it may have a significant impact on the neonate. Please see section 6.1.4 above.
6.2.3. Caesarean section Intravenous antibiotic prophylaxis should be administered to all women.
6.2.4. Vaginal delivery Aseptic precautions should be observed for all operative vaginal deliveries. Prophylactic antibiotics should be prescribed for instrumental vaginal deliveries and repair of 3rd and 4th degree tears.
6.3 Postpartum
- Good personal hygiene & advice to women Provide all women with advice regarding avoiding contamination of the perineum by washing hands before and after using the toilet or changing sanitary pads. It is especially necessary when the woman or her family or close contacts have a sore throat or upper respiratory tract infection.
All women should be informed of the risks, signs and symptoms of infection and the need for them to seek early advice if they are concerned.
- Group A streptococcus See point 6.2.2 intrapartum prevention of sepsis.
- Postnatal temperature: Healthcare professionals carrying out postnatal checks in should have a thermometer to enable them to check the temperature of women who are unwell.
- Communication amongst health care teams
Upon discharge, a proper instruction on antibiotics should be there if the woman required antibiotics during hospital stay, so that appropriate follow-up visits may be arranged and the significance of developing symptoms recognized.
- Prophylactic antibiotics: prophylactic antibiotics for third/fourth degree tears, manual removal of placenta should be prescribed if needed.
7. RECOGNITION OF MATERNAL SEPSIS:
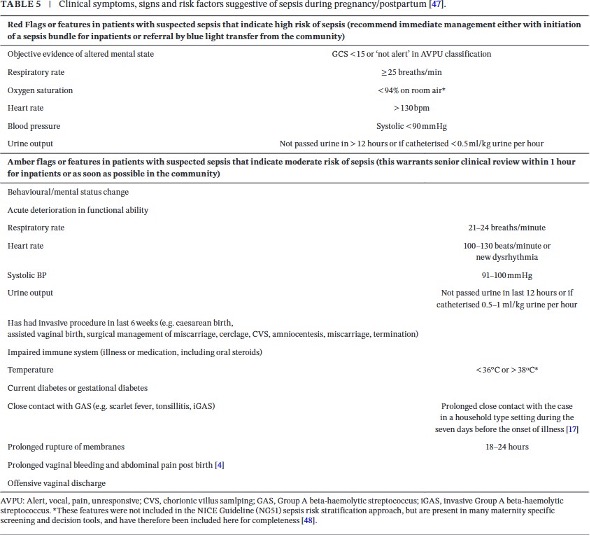
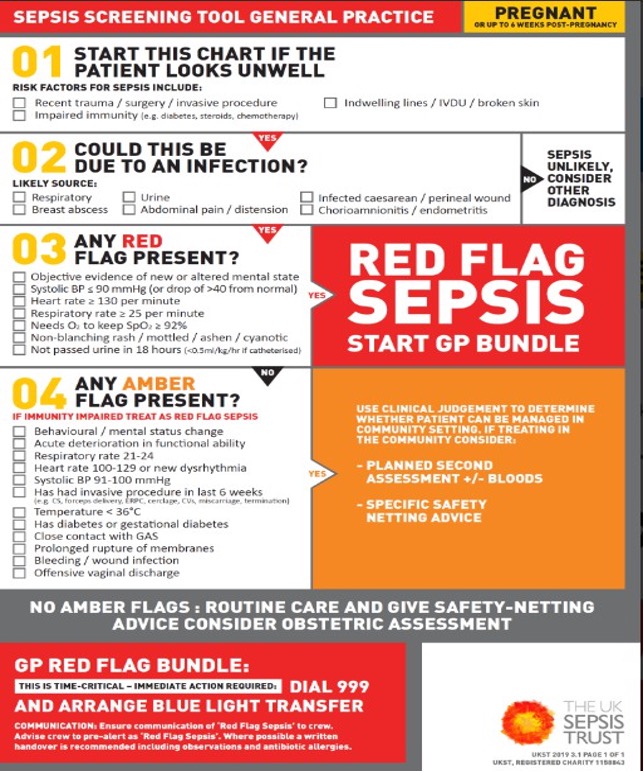
Healthcare professionals should assess all women with suspected infection for maternal sepsis with a risk stratification tool; an example of a sepsis risk stratification tool is given in Appendix3. The possibility of COVID-19 must also be considered, and an assessment for possible COVID-19 conducted in line with current recommendations. Health care providers should be aware of the red flag symptoms and signs of maternal sepsis and of the rapid, potentially lethal course of sepsis and septic shock (Table 5). Disease progression may be much more rapid than in the non-pregnant state.
Appropriate Triggers or Features of Sepsis that should Prompt hospital admission from the Community
The 2023 MBBRACE report recommended “postdelivery, streptococcal infection,
particularly GAS, is most likely to present within 12 hours post- birth. Infection should be suspected and actively ruled out for women who have recently given birth and experience significant abdominal pain or persistent vaginal bleeding. After pains typically reduce in the hours following childbirth and do not develop after dis-charge.
Pain after a vaginal birth that does not settle with simple analgesia should prompt a face-to-face review and a clinical ex-amination including both abdominal and vaginal examination if indicated”
Common Investigations when Sepsis is Suspected
Serum lactate should be measured urgently in women with features indicating a high risk of sepsis to guide care; however, it is recognized that lactate may also be elevated by the physio-logical process of labour and due to other complications common in
pregnancy, such as bleeding. A lactate of 2 mmol/l or more should initiate immediate senior review, intravenous fluid administration and repeat lactate measurement thereafter to gauge response to treatment. Serum lactate of 4 mmol/l or more is indicative of tissue hypoperfusion or cellular metabolic dysfunction. This should prompt immediate escalation of care, including consideration of discussion with critical care regarding ongoing care and intravenous fluid bolus administration.
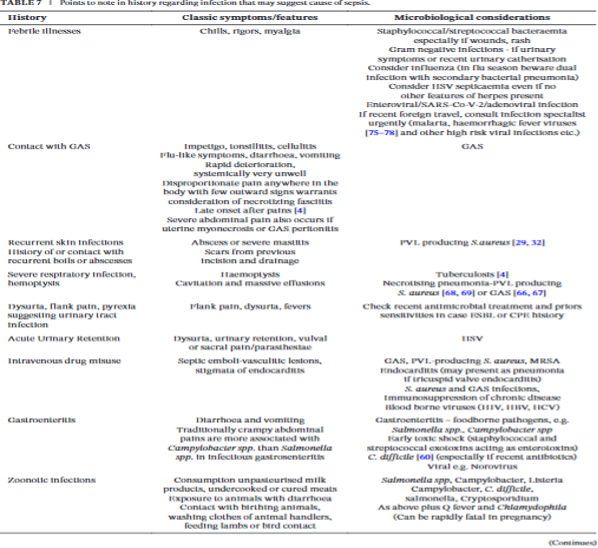
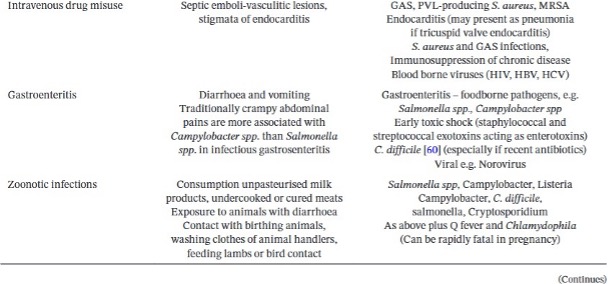
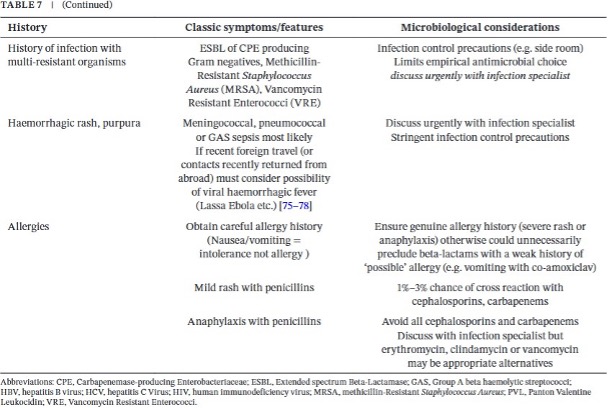
Bacteriology Samples A thorough history can help identify the cause of sepsis (Table
7).Two sets of blood cultures (each set including an aerobic and anerobic bottle) should be taken sequentially, within in minutes of each other. Increasing the volume of blood sampled maximises the aspiration of circulating bacteria and thus the yield of pathogens. Blood cultures should be obtained prior to antibiotic administration and empirical treatment started without waiting for any microbiology results. Consider if a blood sample is indicated for HSV PCR. Other microbiology sampling should be guided
by clinical suspicion of the focus of infection. Where testing is available, a nasal in viral transport media may be sent for rapid MRSA molecular diagnostic screening. The alternative is a pre-moistened nasal swab cultured overnight on selective media. If a woman has a normal CRP or symptoms are more suggestive of a viral respiratory
infection (e.g. SARS-CoV2, influenza) then a viral nasal swab should be taken for PCR. Swabs taken from throat, vagina, caesarean or other wounds should be sent for bacterial culture as appropriate.
Symptoms of tonsillitis/pharyngitis should prompt a throat swab for bacterial culture. Diarrhoea warrants routine stool culture (e.g. Salmonella, Campylobacter) as well as testing for Clostridium difficile toxin, the later especially if diarrhoea follows antimicrobial therapy. An infection specialist should be consulted because of the wide range of highly contagious infections necessitating high-level infection control precautions to protect staff and other patients. The laboratory should be informed if there is a clinical indication for investigations for unusual pathogens eg. consumption of soft cheese or cured meats (Listeria monocytogenes), a history of foreign travel (parasites, malaria, typhoid, cholera, viral haemorrhagic fever, brucella) or hospitalization (multi-drug resistant organism screening).Microbiology results should be reviewed when available to allow optimization of the antibiotic regimen and more targeted therapy. If the woman has been on broad-spectrum antimicrobials before developing signs of sepsis it is likely the pathogen is multi-drug resistant, and an infection specialist should be consulted for ad- vice on further antimicrobial options. Prompt imaging may identify the source of the
infection, allowing early definitive treatment, and should not be deferred on the grounds of pregnancy alone. This could include a chest X-ray and, in women following pregnancy, a pelvic ultrasound scan, computed tomography scan or magnetic resonance im-aging (MRI) scan if pelvic abscess is suspected. In women at moderate risk of sepsis it is suggested clinical examination and results review should be carried out within 1 hour.
Samples for Viral Infection Diagnosis
Women suspected of having influenza should be tested immediately using a viral nasal/throat swab for influenza PCR, barrier nursed and treated with antivirals while awaiting PCR results . Women suspected of SARS- CoV-2 should be assesses according to the RCOG guidance Coronavirus (COVID-19) infection in pregnancy.
8. MANAGEMENT OF RED FLAG SEPSIS
Not all women with red flags will require the sepsis six bundle. A senior clinician may seek an alternative diagnosis and de-escalate care e.g. chronic renal disease or hypertension in pregnancy. Any differential diagnosis and or rationale for not
commencing the sepsis six bundle must be clearly documented. Crucial actions for women with
RED FLAG Sepsis are:
- Early recognition
- Prompt investigation
- Prompt treatment particularly
- Administration of intravenous antibiotics
- Administration of intravenous fluids
- Early involvement of experts & senior review is essential.
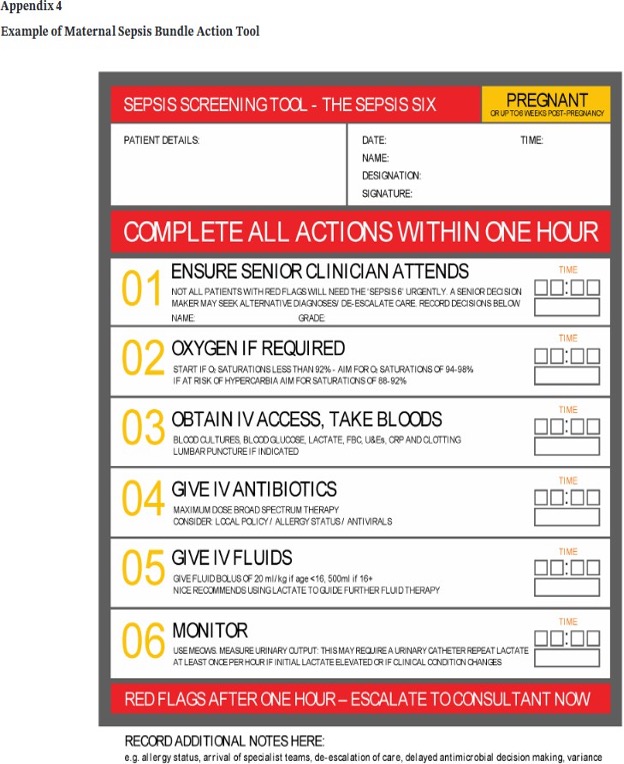
- SEPSIS SIX BUNDLE: THE FIRST HOUR Following completion of the sepsis screening tool and the identification of RED FLAG HIGH RISK FOR SEPSIS (appendix 3) continue with the actions in the sepsis six bundle, (appendix 4). Complete all actions within the hour All women should be transferred to HDU care. Remember – the actions in the sepsis six bundle are only the first stage of management.
ENSURE SENIOR CLINICIAN ATTENDS (SEPSIS SIX BUNDLE: ACTION 1)
In the event of Red Flag Sepsis, all 2 the following staff should immediately attend:
- Senior obstetric registrar
- Obstetric anaesthetic registrar
Early involvement from the following clinicians is crucial, it can save lives and limit morbidity:
- Consultant microbiologist
- Consultant haematologist
- Critical care consultant
If the woman fails to respond within 1 hour of initial antibiotic and/or intravenous fluid resuscitation the on-call Consultant Obstetrician, Consultant Obstetric Anaesthetist (ITU Consultant for out of hours) should attend for decision regarding further supportive management.
Critical care unit should be involved and advice from the Consultant Microbiologist should be urgently sought.
ADMINISTER OXYGEN (SEPSIS SIX BUNDLE: ACTION 2)
Monitor and maintain airway, breathing, circulation as your first priority. Administer high flow oxygen by facemask with a reservoir bat at 15L/minute.
Aim to keep oxygen saturations above 94%. If the woman is at risk of carbon dioxide retention i.e. chronic obstructive pulmonary disease or Type 2 Respiratory Failure, aim for oxygen saturations of 88-92%.
OBTAIN IV ACCESS TAKE BLOODS (SEPSIS SIX BUNDLE: ACTION 3)
Secure intravenous access as soon as possible, blood samples should include those detailed in the table:
| Blood samples to obtain for investigation | |
| Blood cultures DO NOT DELAY THE ADMINISTRATION OF ANTIBIOTICS | Peripheral sample collection of blood culture specimens If the woman has central venous catheter (CVC) or any central line, then a sample should be taken as well from these lines if suspected for infection. |
| Serum lactate | Women with severe sepsis or septic shock typically have a high serum lactate which may be secondary to anaerobic metabolism attributable to poor tissue perfusion. A lactate of ≥ 4 mmol/L indicates a poor prognosis & should trigger a referral to critical care. If the serum lactate is ≥ 4 mmol/L or there is suspected hypovolemia due to the sepsis administer an initial fluid challenge of 500 mL crystalloid in 15 minutes regardless of blood pressure. This fluid challenge is recommended because of the high risk of septic shock. If there is no improvement of the serum lactate with the Sepsis Six, the woman should be transferred to critical care for possible vasopressor support. |
| Full blood count | White blood cells (WBC) are commonly raised (more than 14 x 109 /L) with a high neutrophil count in sepsis. However the WBC can also be low (less than 4 x 109 /L). |
| Renal & liver function | Acute tubular necrosis may develop which can lead to renal failure with raised urea, creatinine, and potassium levels. The pro- inflammatory state of sepsis can also lead to hyper bilirubinaemia and jaundice. |
| C-reactive protein (CRP) | CRP is an inflammatory marker, commonly raised during infection. Monitoring the trend can be a useful guide a response to the treatment of infection. |
| Clotting studies | Disseminated intravascular coagulation (DIC) is a potential complication of sever sepsis. |
| Take blood for activated partial thromboplastin time (APTT), prothrombin and fibrinogen. Communicate with the on-call haematologist if the investigation results are abnormal. The administration of platelets, fresh frozen plasma, & or cryoprecipitate /fibrinogen concentrate may be indicated. | |
| Arterial blood gas (ABG) | An ABG is very useful in any woman who is unwell. It is likely to show acidaemia (arterial pH less than 7.35). This is typically a metabolic acidosis secondary to lactate production. |
GIVE INTRAVENOUS ANTIBIOTICS (SEPSIS SIX BUNDLE: ACTION 4)
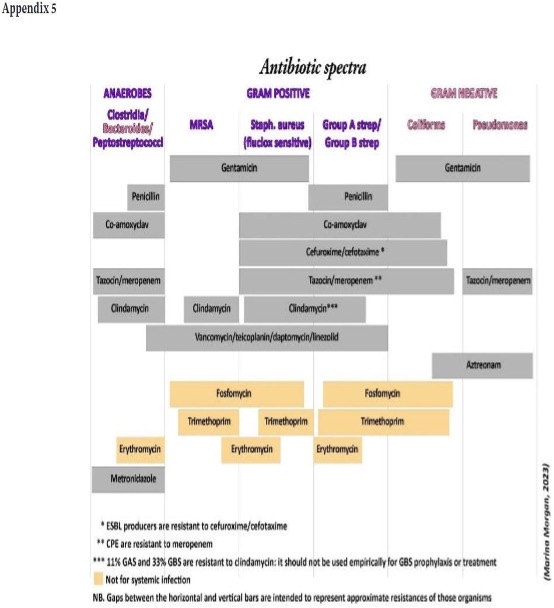
Administer immediate high dose broad-spectrum intravenous antibiotic therapy. See appendix 6 antimicrobial guidance. Consider the need for anti-retroviral medication. DO NOT DELAY THE ADMINISTRATION OF ANTIBIOITCS WHILST WAITING FOR
INVESTIGATION RESULTS. If possible, obtain blood cultures prior to the antibiotics being administered but these should not delay antibiotic administration. Early involvement of the microbiologist is crucial.
GIVE INTRAVENOUS FLUIDS (SEPSIS SIX BUNDLE: ACTION 5)
An initial fluid challenge of 500 mL crystalloid in 15 minutes should be administered. The woman may require up to 30 mL/kg of intravenous fluids. This means a 70 kg woman with sepsis should receive 2 litres of intravenous crystalloid.
- If lactate ≥2mmol/L give 500mL stat.
- If hypotensive or lactate ≥ 4mmol/L can repeat boluses up to 30mL/kg (e.g. 2L for a 70 kg woman)
Extreme caution must be exercised in women with pre-eclampsia/suspected or confirmed heart failure. Liaise closely with the Consultant Obstetrician /Anaesthetist team and critical care.
MONITOR (SEPSIS SIX BUNDLE: ACTION 6)
This includes accurate measurement of the urine output.
Women with maternal sepsis can deteriorate rapidly. Extreme vigilance with observations and assessment is crucial. Record all observations on a high dependency care chart & MEOWS.
Commence the high dependency care (HDC) chart in the location where sepsis RED FLAG triggers are identified i.e. if identified on the wards then commence HDC chart prior to transfer to delivery suite.
If the woman is on the ward, transfer to delivery suite for the provision of high dependency care. Consider the need to transfer to critical care
Early advice from an infectious diseases physician or microbiologist should be sought; this is essential in instances where the woman fails to respond to the first- choice antibiotic.
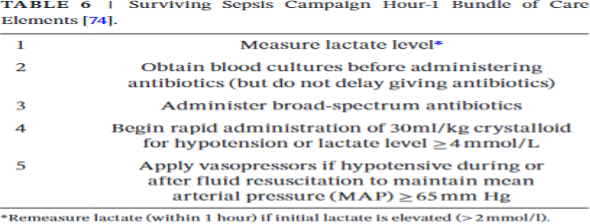
Table 5 Monitoring & observations in maternal sepsis
| Monitoring & observations in maternal sepsis | |
| Monitor | Frequency |
| Respiratory rate Pulse rate Blood pressure Oxygen saturations | Every 15 minutes until stabilized and then every 30 minutes. Tailor according to treatment response |
| Temperature | At least 4 hourly |
| Urine output | Hourly by Foley’s catheter |
| Blood samples | Full Blood CountUrea & ElectrolytesLiver Function TestsSerum lactateBicarbonateGlucoseMagnesium, phosphate & calcium Every 4-12 hours dependent upon clinical situation |
| Fetal heart rate | monitoring with a CTG if appropriate |
- Further management of sepsis
- Continue with the observations detailed in table 6
- Serial lactates will assess a response to treatment.
- Stop non-steroidal medicines as these are contraindicated in sepsis.
- Removing the source of the infection
- Identify the source of sepsis and remove as soon as the woman is stable.
- Perform a full ‘top to toe’ clinical examination with the aim of identifying the cause of the sepsis.
- Include a vaginal examination to exclude retained swab or tampon.
- Swabs or cultures listed below should be obtained from all potential sources of sepsis & sent for urgent microbiology investigation:
- Vaginal & wound swabs
- Urine culture
- Throat swab
- Stool sample
- Sputum sample
- Placental swab (if immediately postpartum)
- Removing the source of the infection
The results of all investigations must be followed up and antibiotic treatment altered accordingly
Imaging may help to identify the source of infection
- Chest X-ray o Abdominal ultrasound
- CT of chest, abdomen pelvis
- Expedite delivery if there are signs of chorioamnionitis to aid resuscitation measures; liaise with the neonatologist.
- Retained products of conception: remove retained products as soon as the woman is stable.
- Closed-space infections need surgical drainage.
- In women with endometritis not responding to antibiotics, consider septic pelvic thrombosis.
- Necrotizing fasciitis requires early surgical intervention with fasciotomy and aggressive antibiotic therapy.
- Venous thromboembolism prophylaxis
- Deep vein thrombosis prophylaxis with low molecular weight heparin and the use of compression stockings should be considered
- Venous thromboembolism prophylaxis
9. DETERIORATING WOMEN WITH SEPSIS
If the woman fails to respond within 1 hour of initial antibiotic and/or intravenous fluid resuscitation
The on-call Consultant Obstetrician, Consultant Obstetric Anaesthetist (ITU Consultant for out of hours) should attend for decision regarding further supportive management +/- transfer to critical care unit.
- Immediate involvement of Critical Care Team
- Advice from the Consultant Microbiologist should be urgently sought.
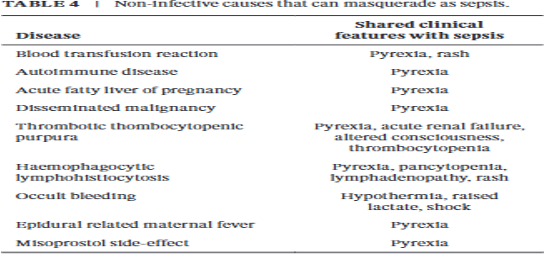
- Consider other conditions mimicking sepsis especially when not responding to treatment. This includes:
- Occult haemorrhage (concealed gastrointestinal bleeding)
- Myocardial infarction
- Adrenal insufficiency
- Venous thrombosis.
- Signs of septic shock Sepsis and (despite adequate volume resuscitation) both of:
- Persistent hypotension requiring vasopressors to maintain Mean Arterial Pressure (MAP) greater than or equal to 65 mm Hg, and
- Lactate greater than or equal to 2 mmol/l (despite fluid resuscitation). Pragmatically and usually as a trigger to call Critical Care, a woman who is hypotensive (Red Flag criterion, systolic blood pressure (SBP)
- Multi-disciplinary team management of Septic Shock/Severe Sepsis
- Follow resuscitation measures of airway, breathing and circulation.
- Seek advice from Consultant Microbiologist and consider additional or alternative IV antibiotics.
- Repeat microbiological specimens and mark ‘urgent’.
- MDT involvement as in section 9 above to arrange for the transfer of the woman to critical care.
Compiled By:
Dr. Tasrina Hamid
Contributors :
- Prof Fawzia Hossain
- Dr Mirza Mohd Asaduzzaman
- Dr Sumaiya Binte Asif
- Dr Maniza Khan
- Dr Taslima Akter Tithi
- Dr Tasnuva Akter
- Dr Tuli Akter
- Dr Jesmin Akter
- Dr Fahmida Jesmin
- Dr Amena Fardous
