

The Robson Classification is for “all women” who deliver at a specific setting and not only for the women who deliver by CS.
Aims and objectives of RTGC
WHO expects that the use of the Robson Classification will help health care facilities to:
• Identify and analyses the groups of women which contribute most and least to the overall CS rates.
• Compare practice in these groups of women with other units that have more desirable results and consider changes in practice.
• Assess the effectiveness of strategies or interventions targeted at optimising the use of CS.
• Assess the quality of care and of clinical management practices by Analysing outcomes by groups of women.
• Assess the quality of the data collected and raise staff awareness about the importance of this data, interpretation and use.
Why is the rise in caesarean section a concern?
When the caesarean delivery rate–as a percentage of live births–has been rising globally, there is growing concern about unnecessary caesarean sections.
Unnecessary caesarean sections can increase the risk of maternal morbidity, neonatal death, and neonatal admission to an intensive care unit. To understand the drivers of this trend and to propose and implement effective measures to regulate CS rates where needed, it is necessary to have a tool to monitor and compare CS rates in the same setting over time and between different settings.
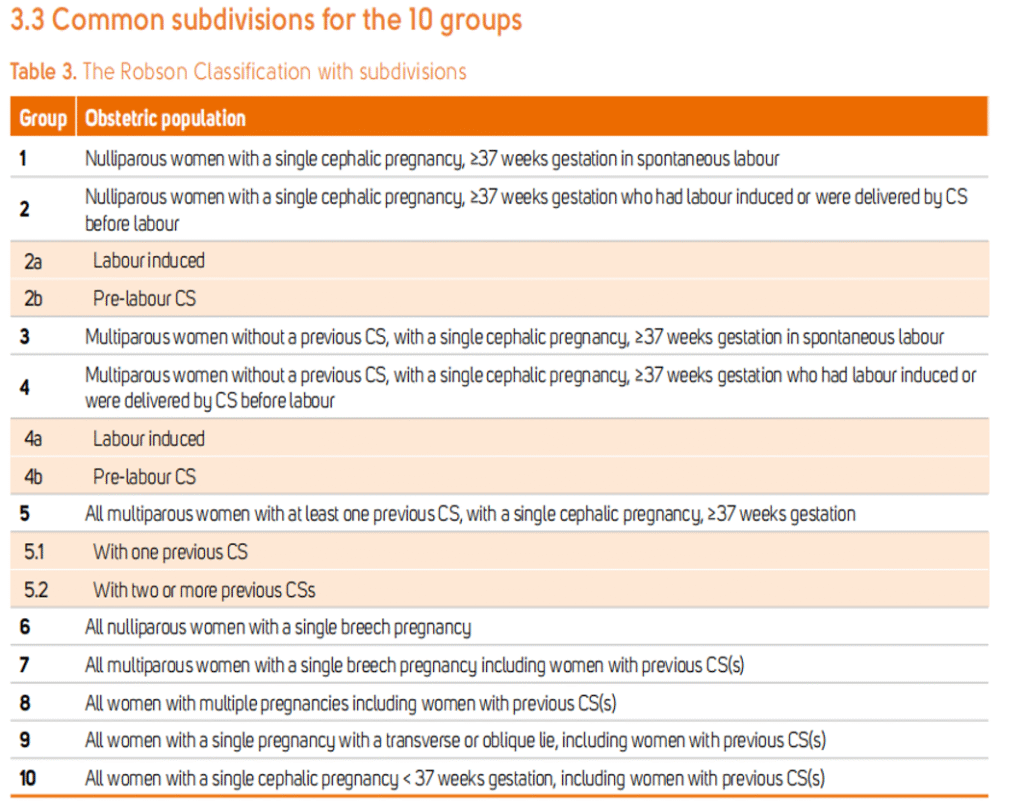
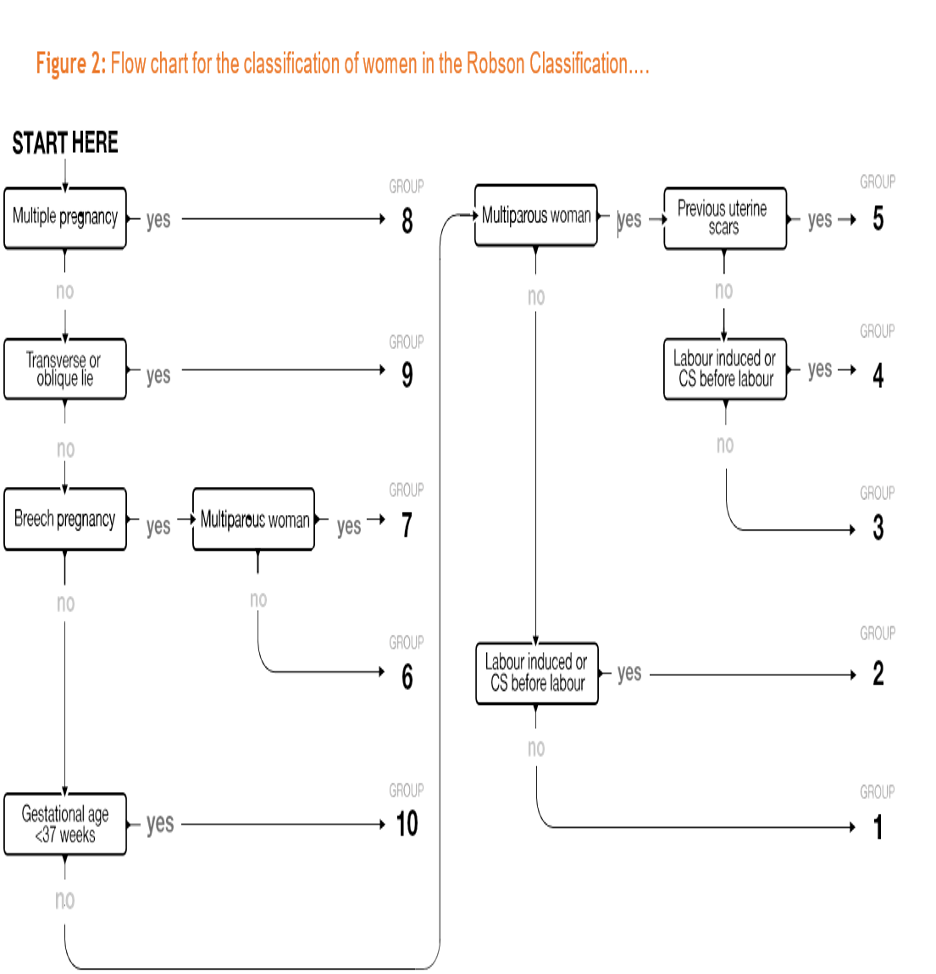
The 10 groups of the Robson Classification
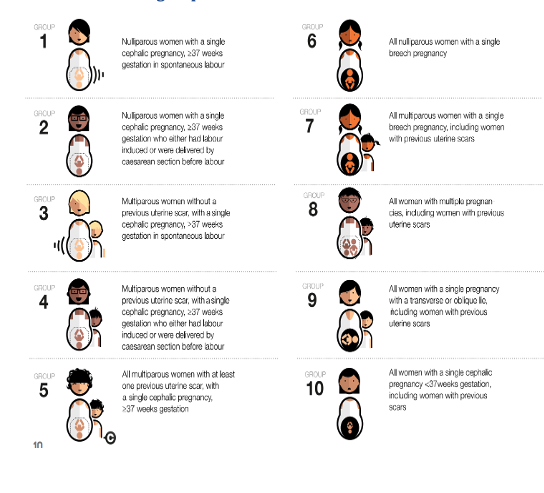
The 10 groups are based on six basic obstetric variables; these are the only information needed to classify each woman:
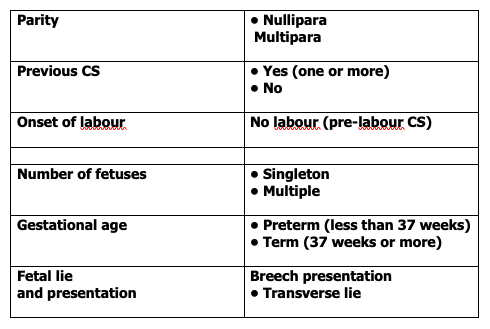
| Group | Parity | Previous CS | Number of fetuses | Fetal presentation or lie | Gestational age (weeks) | Onset of labour |
|---|---|---|---|---|---|---|
| 1 | 0 | No | 1 | Cephalic | ≥ 37 | Spontaneous |
| 2 | 0 | No | 1 | Cephalic | ≥ 37 | Induced or CS before labour |
| 3 | ≥ 1 | No | 1 | Cephalic | ≥ 37 | Spontaneous |
| 4 | ≥ 1 | No | 1 | Cephalic | ≥ 37 | Induced or CS before labour |
| 5 | ≥ 1 | Yes | 1 | Cephalic | ≥ 37 | Any |
| 6 | 0 | No | 1 | Breech | Any | Any |
| 7 | ≥ 1 | Any | 1 | Breech | Any | Any |
| 8 | Any | Any | ≥ 2 | Any | Any | Any |
| 9 | Any | Any | 1 | Transverse or Oblique | Any | Any |
| 10 | Any | Any | 1 | Cephalic | < 37 | Any |
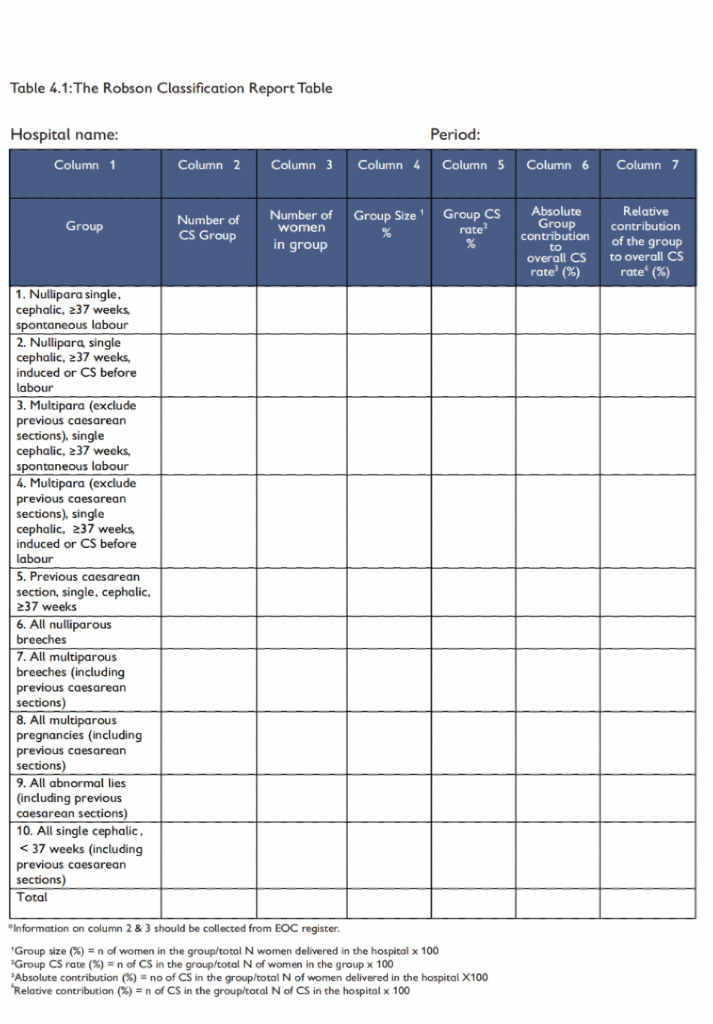
The Report Table
The Report Table consists of seven columns as follows:
| Column | Description |
|---|---|
| Column 1 | Group name and/or number and definition (with subdivisions for Groups 2, 4 and 5, if these are of interest to the users) |
| Column 2 | Total number of CS in each group |
| Column 3 | Total number of women delivered in each group |
| Column 4 | Relative group size to overall facility population. For each of the 10 groups, in percentage |
| Column 5 | CS rate in each group. For each of the 10 groups, in percentage |
| Column 6 | Absolute group contribution to overall CS rate. For each of the 10 groups, in percentage |
| Column 7 | Relative contribution of each of the 10 groups to overall CS rate. For each of the 10 groups, in percentage |
Definition of core variables used in the Robson Classification
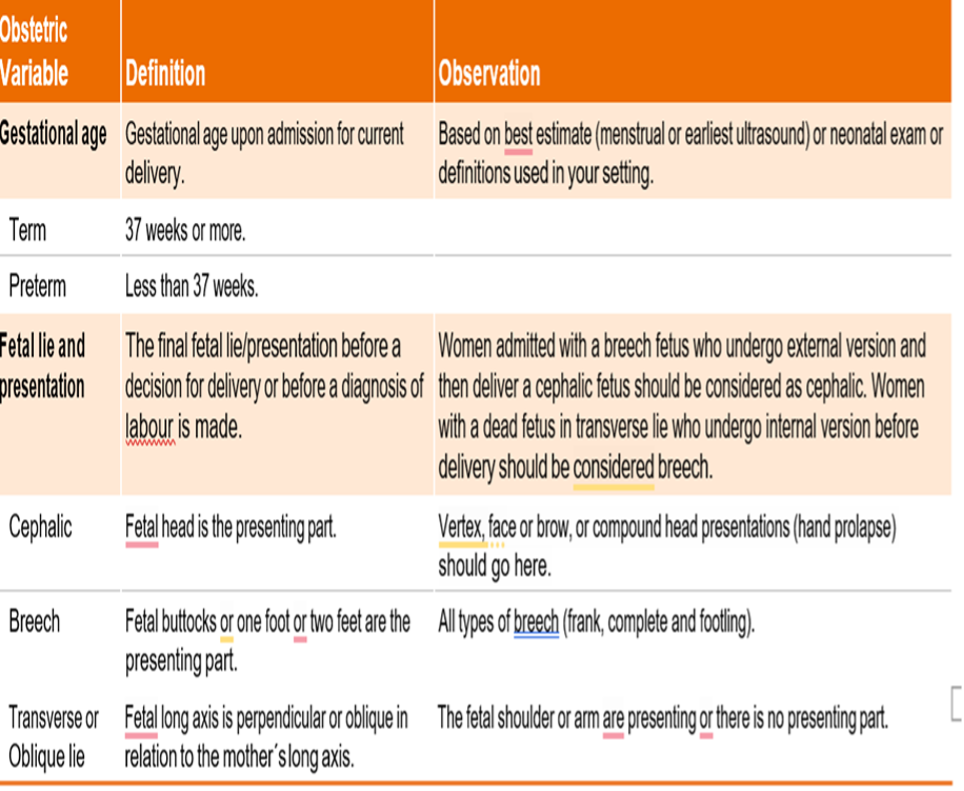
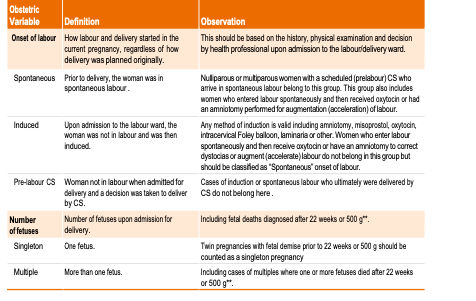
(The original text did not provide details here, so it is retained as a placeholder.)
Robson’s Ten Group Classification with probable interventions
| Group | Description | Intervention |
|---|---|---|
| 1 | Nulliparous, single cephalic, ≥37 weeks, in spontaneous labour. | 1.1 ANC Counseling on the importance of VD. 1.2 Explaining the pregnant woman during ANC what to expect/what will happen during the process of labour and delivery; avoiding indication of CS. 1.3 Respectful maternity care. 1.4 Supportive care during labour. 1.5 Differentiate between active phases of labour. 1.6 Consider latent phase up to 6h and go on partograph after 5 cm. 1.7 Dystocia: Diagnosed by Partograph. 1.8 Augmentation by medical method (oxytocin) or ARM (if need augmentation) and cut short 2nd stage (AVD). 1.9 Epidural anaesthesia / labour analgesia. |
| 2 | Nulliparous, single cephalic, ≥37 weeks, induced or CS before labour. | |
| 2a | Induced labour. | Perform modified Bishop Score, Induction according to score, Exercise to labouring women. |
| 2b | Pre-labour C-section. | Good antenatal counselling about the benefits of vaginal delivery, explaining the pregnant woman during ANC what to expect/what will happen during the process of labour and delivery. Exercise for labouring women. |
| 3 | Multiparous (excluding previous caesarean section), singleton, cephalic, ≥37 weeks’ gestation, in spontaneous labour. | 1.1 Admission to labour unit, intrapartum phase of labour, and supportive care. 1.2 Exercise for labouring women. 1.3 If needed, augmentation and cut short the 2nd stage (AVD). 1.4 Epidural anaesthesia/labour analgesia. |
| 4 | Multiparous without a previous uterine scar, with singleton, cephalic pregnancy, ≥37 weeks’ gestation, induced or caesarean section before labour. | Good antenatal counselling about the benefits of vaginal delivery, explaining the pregnant woman during ANC what to expect/what will happen during the process of labour and delivery. Exercise for labouring women. |
| 4a | Induced labour. | Perform modified Bishop Score, Induction according to score. |
| 4b | Pre-labour C-section. | Good antenatal counselling about the benefits of vaginal delivery. Exercise to labouring women. |
| 5 | Multiparous with at least one previous caesarean section, singleton, cephalic, ≥37 weeks’ gestation. | |
| 5a | With one previous C-section. | Encourage VBAC with good screening and careful monitoring. |
| 5b | With two or more previous C-sections. | Elective, repeat C-section. |
| 6 | All nulliparous with a single breech. All multiparous with a single breech (including previous caesarean section). | External Cephalic Version (ECV) if possible. |
| 7 | All multiparous with a single breech and no previous caesarean section. | ECV or allow spontaneous labour for vaginal delivery. |
| 8 | All multiple pregnancies (including previous caesarean section). | ✓ Multiple pregnancies with a previous one or more CS: allow CS. ✓ Multiple pregnancies with no previous CS: may allow CS. ✓ Multiple pregnancies with malpresentation and/or severe medical complications: allow caesarean delivery. |
WHO recommendation on interventions targeted at women for the reduction of unnecessary caesarean sectionsyes
Child-birth training and workshops
- Training comprised three four-hour weekly sessions in groups of 30 members.
- Content includes counseling on fear of childbirth and pain, pharmacological pain-relief techniques and their effects, nonpharmacological pain-relief methods, advantages and disadvantages of caesarean and vaginal delivery, and indications and contraindications of caesareans.
A nurse-led ‘applied relaxation’ training program
- The program comprised seven, 90-minute, group education sessions over seven weeks led by a nurse, under the supervision of a clinical psychologist.
- Content includes group discussion of anxiety and stress-related issues in pregnancy and the purpose of applied relaxation and deep breathing techniques, among other relaxation techniques.
Psychosocial couple-based prevention program
- The psychosocial program comprised nine classes, with four weekly classes conducted during the second or third trimester of pregnancy and four weekly classes conducted within the first six months postpartum.
- Classes focus on emotional self-management, conflict management, problem-solving, communications, and mutual support strategies that foster positive, joint-parenting of an infant.
- ‘Couple’ in this recommendation includes couples, people in a primary relationship, or other close people.
Psychoeducation for women with fear of childbirth
- The psychoeducational group therapy was led by four different psychologists with special group therapeutic skills in pregnancy-related issues. Six group sessions were held during pregnancy and one was held with the newborns six to eight weeks after delivery.
- Each two-hour session comprised a focused topic and a 30-minute guided relaxation exercise using an audio recording developed for this purpose. This relaxation exercise guided the participants through stages of imaginary delivery in a relaxed state of mind with positive, calming, and supportive suggestions.
- The topics covered included information about fear and anxiety, fear of childbirth, normalization of individual reactions, stages of labour, hospital routines, the birth process, and pain relief.
Conclusion
The TGCS represents a new way of thinking. It is not just a classification of cesarean delivery or a useful way of focusing on how to reduce cesarean delivery rates.
It provides a common starting point for further analyses of all labour and delivery events and outcomes, and its principles of simplicity and clarity of thought help to stimulate interest, discussion, and education. Significantly, it is presented in such a way that all clinicians, irrespective of their academic or professional background, can identify it, encouraging long-term commitment and responsibility, especially when shared nationally and internationally.
If the hospitals and health organizations use the TGCS, it would allow standardized comparisons of cesarean delivery rates by identifying prospectively clinically distinct groups of women that are driving cesarean delivery rates.
It would also allow for a more targeted evaluation of the quality and the processes associated with cesarean delivery in these different groups.
Compiled By:
Dr. Munawar Sultana
Contributors
- Prof Fawzia Hossain
- Prof Maruf Siddique
- Prof Firoza Begum
- Dr Taslima Akter
- Dr Maniza
- Dr Rafa
- Dr Sumaiya Binte Asif
- Dr Lata Dutta
- Dr Amrita Saha
- Dr Raunak Jahan
- Dr Israt Jahan
- Dr Farzana Bithi
- Dr Tahera
- Dr Tania Akter
