

Prepared By : DR. Tasrina Akter
Scope (Target audience): Clinicians, Gynaecologists
Review date: October 2005
Patient group to which it applies: This guideline should be applied to all gynaecological patients admitted for surgery, and to all early pregnancy inpatient patients.
NICE guidance reference: N/A
Summary of evidence base: This guidance has been created from TOG article Volume 25, Issue 1
Contents
- Introduction
- Pathophysiology of thrombosis
- Thromboprophylaxis in early pregnancy
- Thromboprophylaxis in gynaecological surgeries
- Modes of thromboprophylaxis
- Complications of VTE
- Contraindications and complications of thromboprophylactic measures
- Table 1
- Table 2
1. INTRODUCTION
Venous thromboembolism (VTE) is a major cause of morbidity and mortality. It is a largely preventable complication following surgery. Without thromboprophylaxis, the incidence of confirmed deep vein thrombosis (DVT) in major abdominal surgery ranges from 17 to 40%. The risk of VTE following surgery exists for the first 12 weeks, with the likelihood of admission with VTE being greatest in the first 6 weeks. Hospital-acquired, or hospital-associated, thrombosis (HAT) is defined as any venous thromboembolic event occurring in hospital or within 90 days of hospital admission. This accounts for 50–60% of all thromboembolic events.
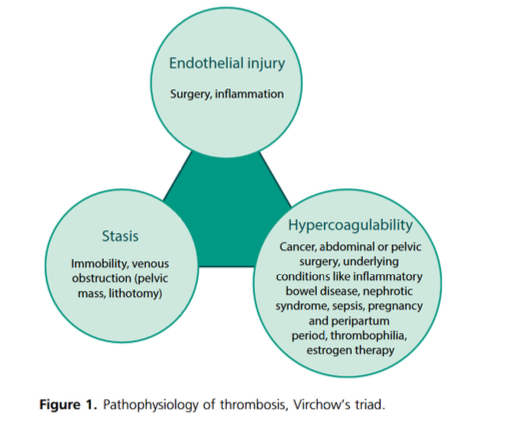
2. PATHOPHYSIOLOGY OF THROMBOSIS
The basis for thrombosis is explained by the Virchow’s triad: endothelial injury; stasis; and hypercoagulability. Risk factors can be identified in relation to each of these three components.
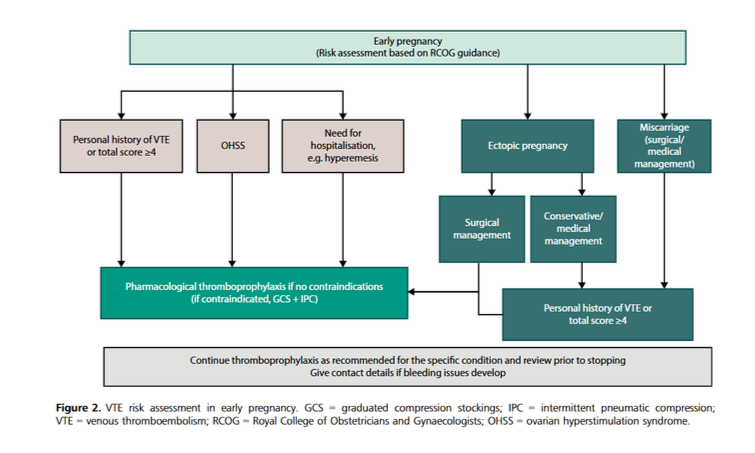
3. THROMBOPROPHYLAXIS IN EARLY PREGNANCY
The risk for VTE increases from the first trimester. This is attributed to the hypercoagulable state in pregnancy. Thrombin generation increases in women as early as 5 weeks of gestation.
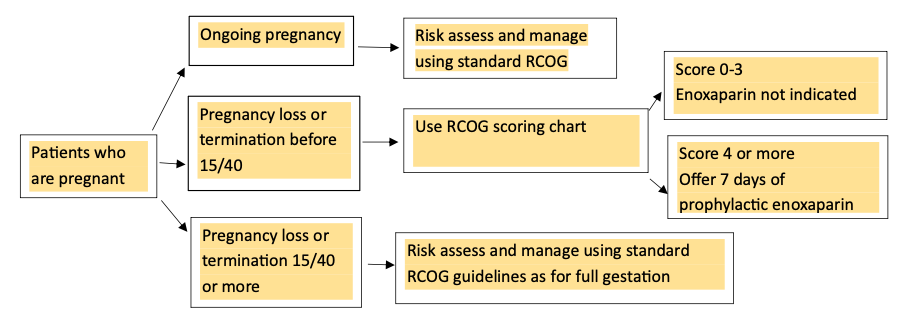
Ongoing pregnancy: Risk assess and manage using standard RCOG guideline. Score 0-3 → Enoxaparin not indicated
Pregnancy loss or termination before 15/40: Use RCOG scoring chart. Patients who Score 4 or more → Offer 7 days of prophylactic enoxaparin
Pregnancy loss or termination 15/40 or more: Risk assess and manage using standard RCOG guidelines as for full gestation
Risk with hyperemesis and ovarian hyperstimulation syndrome (OHSS): Hyperemesis is a recognized risk factor for VTE, primarily associated with dehydration and resulting haemoconcentration. Immobility caused by fatigue may further increase the risk. This is a transient risk existing during the period of hyperemesis. OHSS also has a clear link to VTE. Rova et al. showed a 100-fold increased risk of VTE in pregnancies achieved by in vitro fertilization (IVF) and complicated by OHSS, as opposed to a five-fold increased risk in IVF pregnancies without OHSS. There are some risks of VTE with miscarriage and ectopic pregnancy. So, risk should be assessed and managed accordingly.
4. THROMBOPROPHYLAXIS IN GYNAECOLOGICAL SURGERIES
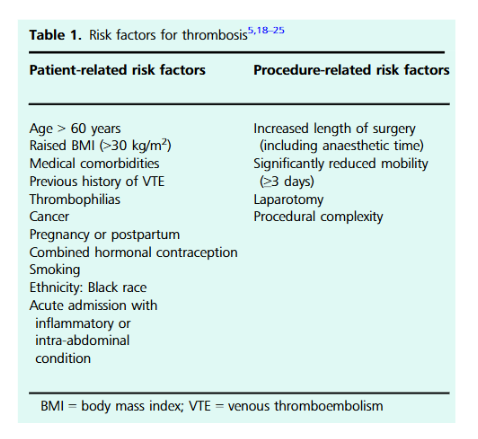
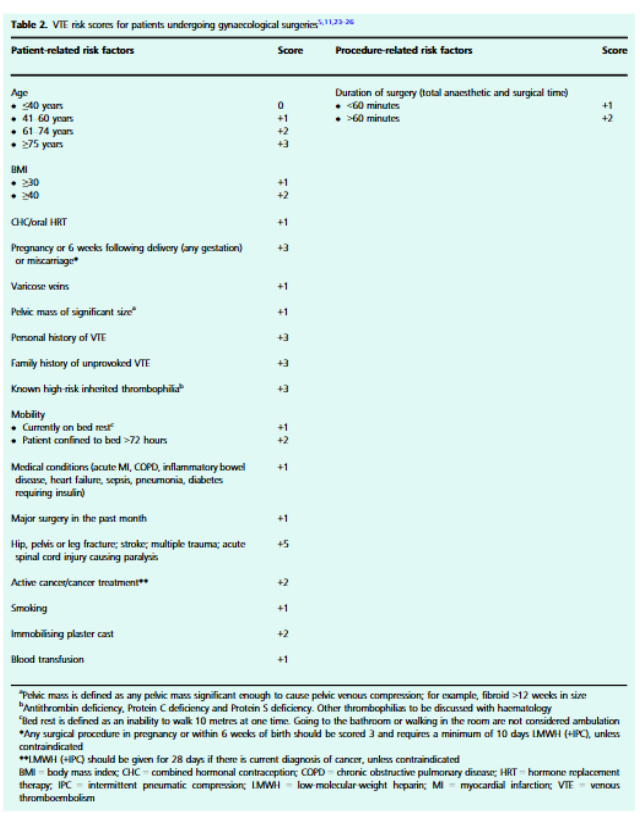
Various studies have identified factors associated with increased risk of VTE following surgery. Broadly, these can be classified into patient-related and procedure-related risk factors.
Patient related risk factors:
- Risks with underlying malignancy: Cancer is a risk factor for VTE. In gynaecological cancer patients undergoing surgery, there is a significantly higher risk of VTE in the postoperative period for those undergoing laparotomy than laparoscopy.
- Risk of Combined hormonal contraception (CHC): CHC should be stopped 4 weeks before elective surgery and only restarted at least 2 weeks after regaining full mobility following surgery. A progesterone-only contraceptive may be offered as an alternative. In emergency surgical situations, when the patient is on CHC, thromboprophylaxis should take this into account as an additional risk factor.
- Risks with hormone replacement therapy (HRT): A study by Vinogradova et al. showed that transdermal HRT is safest in the context of VTE with no increased risk of VTE with different regimens. The overall risk of VTE is not increased by continuing HRT in the perioperative period. The Society of Obstetricians and Gynaecologists of Canada (SOGC) guidelines on prevention of venous thromboembolic disease in gynaecological surgery recommend no cessation of HRT before surgery. Instead, HRT should be considered within the VTE risk-assessment for surgery.
- Thromboembolic risk with COVID-19: COVID-19 has been identified as a risk factor for VTE. The associated hypercoagulability must be considered when planning surgery for patients currently or recently affected by COVID-19.
Procedure-related risk factors:
- Effects of anaesthesia and length of surgery: VTE increased progressively with increasing duration of surgery. There is some evidence that regional anaesthesia is associated with a lower risk of VTE than general anaesthesia. NICE guidance [NG89] suggests considering regional anaesthesia in suitable patients as an additional thromboprophylactic measure.
- Route of surgery: Laparotomy versus laparoscopic surgery: Hysterectomy for benign pathology showed a higher incidence of VTE with laparotomy than laparoscopy. Similar results were shown when analysing hysterectomy for endometrial cancer, with increased VTE rates with laparotomy than laparoscopic and vaginal routes of surgery. In surgeries other than hysterectomy (adnexal pathology, ovarian cyst, endometriosis, infertility), no increased risk of VTE was found with laparoscopy.
- Route of surgery: Vaginal versus abdominal: Vaginal surgery is associated with very low rates of VTE.
5. MODES OF THROMBOPROPHYLAXIS
- Early ambulation, hydration
- Mechanical: anti-embolic stockings/graduated compression stockings (GCS)
- Mechanical: intermittent pneumatic compression (IPC)
- Pharmacological thromboprophylaxis: LMWH, LDUH (low dose unfractionated heparin), Fondaparinux, DOAC (Direct oral anticoagulant)
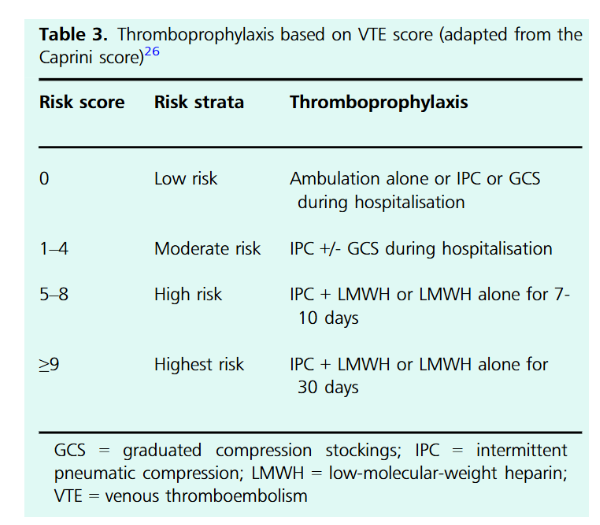
All patients admitted for surgery should have a VTE risk assessment completed within 24 hours of admission.
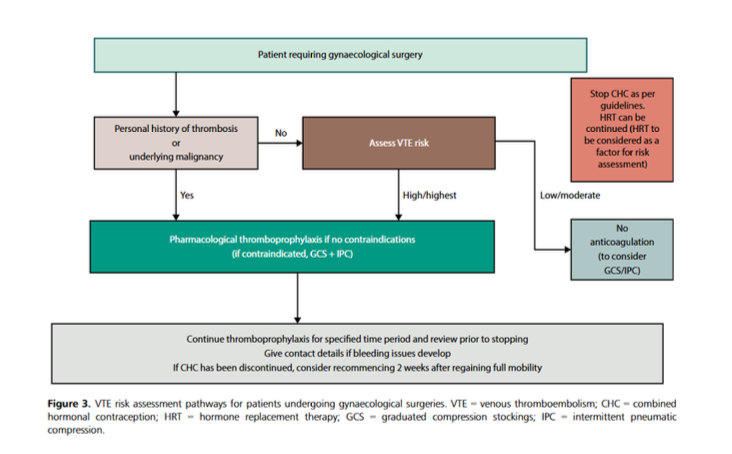
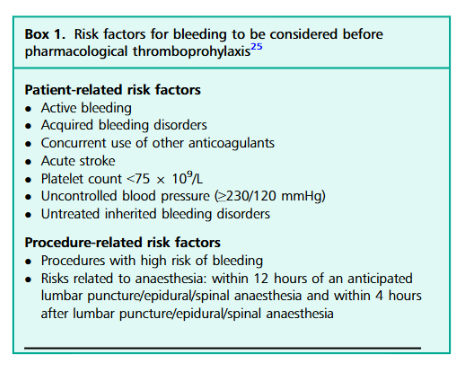
If the risk of VTE is higher than the risk of bleeding, pharmacological thromboprophylaxis is indicated. Patients with a previous personal history of VTE should be offered pharmacological thromboprophylaxis unless contraindicated. 28 days post-operation for most Gynae Oncology patients – if not sure please check with the team. Dose might be increased depending on weight.
Offer enoxaparin prophylaxis for a minimum of 7 days for other gynaecological pelvic surgery. Duration of extended thromboprophylaxis should start from the day of operation and include days spent as inpatient at the same dose/regime as during admission.
Dose for Pharmacological prophylaxis: weight based
- Weight below 50kg → Enoxaparin 20 mg once daily
- Weight 50-100 kg → Enoxaparin 40 mg once daily
- Weight 101-150 kg → Enoxaparin 40 mg twice daily
- Weight above 150 kg → Enoxaparin 60 mg twice daily
- Fondaparinux 2.5 once daily (if heparin allergy/HIT or if patient declines porcine products)
6. COMPLICATIONS OF VTE
The most serious complication of VTE is death caused by pulmonary embolism. Another common but under-recognized complication is post-thrombotic syndrome, which can affect up to 50% of patients in the first 2 years after a diagnosis of DVT. This presents with leg swelling, pain, hyperpigmentation and thickening of the skin, leg ulcers, and venous gangrene.
7. CONTRAINDICATIONS AND COMPLICATIONS OF THROMBOPROPHYLACTIC MEASURES
Mechanical thromboprophylaxis
- Anti-embolic stockings are contraindicated in: Peripheral arterial disease, peripheral arterial bypass grafting, peripheral neuropathy, skin conditions like dermatitis, conditions where the stocking may further damage the skin (leg oedema, severe limb deformity), known allergy to the material
- Intermittent pneumatic compression is contraindicated in: Allergy to the material of the compression sleeve, localized leg problems like cellulitis, wound infection, oedema from congestive heart failure, venous problems like active phlebitis or DVT, significant arterial insufficiency
Pharmacological thromboprophylaxis
- Offer enoxaparin prophylaxis for a minimum of 7 days following abdominal surgery.
- Consider extended enoxaparin prophylaxis for 28 days following major cancer surgery in the abdomen.
Compiled By:
DR. Tasrina Akter
Contributors :
- Prof Fawzia Hossain
- Prof Anowara Begum
- Prof Sayeba Akter
- Dr Sumaiya Binte Asif
- Dr Maniza Khan
- Dr Taslima Akter Tithi
- Dr Reshma Sharmin
- Dr Suraiya Binte Azar
- Dr Tanjila Karim
- Dr Anannya Zakia
- Dr Aklima Zinan
